Abstract
Gambling disorder (GD) is a behavioral addiction that reduces an individual’s quality of life, is associated with feelings of loneliness, and is negatively influenced by object relations. This study aimed to examine the relationships between GD, object relations, loneliness, and quality of life. This research primarily seeks to understand the etiological foundations of GD by analyzing the direct and indirect effects of object relations-related factors on GD using structural equation modeling.
The study was conducted with 443 participants living in Turkey, who were included in an online survey. The data were analyzed using structural equation modeling. The indirect effect of object relations on GD via the mediating role of loneliness was found to be significant (β = .169, p < .001). Reality testing was found to have both a direct and indirect effect via the mediating role of loneliness on GD (β = .030, p < .05). The findings indicate that impairments in object relations increase feelings of loneliness and indirectly influence the severity of GD. The findings also highlight the importance of addressing loneliness and impaired reality testing in therapeutic interventions for GD. The results suggest that the current study contributes to the literature by providing insights into the psychodynamic and psychosocial factors associated with GD.
Keywords: gambling disorder, object relations, loneliness, quality of life, reality testing, behavioral addiction
Main Points
- Gambling disorder is significantly associated with impairments in object relations, loneliness, and deterioration in quality of life.
- Loneliness is a key mediating variable that explains the indirect effect of impairments in object relations on gambling disorder.
- Reality testing affects gambling disorder both indirectly through loneliness and directly.
- Quality of life decreases as the severity of gambling disorder increases.
Introduction
Gambling refers to risking money or valuables on uncertain outcomes and encompasses various forms such as lotteries, sports betting, casino games, card games, and online platforms (Ferentzy & Turner, 2013). The rapid expansion of online gambling in recent decades has increased accessibility and elevated the risk of addiction, prompting public health systems to expand prevention and intervention efforts. In recognition of its addictive nature, the DSM-5 classifies Gambling Disorder (GD) under “Substance-Related and Addictive Disorders,” citing neurobiological and behavioral similarities to substance use disorders (American Psychiatric Association [APA], 2013). A GD diagnosis requires persistent and recurrent gambling behavior that causes significant distress or functional impairment.
The global prevalence of GD varies across populations and methodologies, yet existing evidence suggests that it constitutes a serious public health concern. A recent meta-analysis reported that 2.43% of adults engage in at-risk gambling and 1.29% meet criteria for problem gambling (Gabellini et al., 2022). National-level data show consistent patterns: In the UK, GD affects 0.5% of the population, with higher prevalence among men (1.0%) than women (0.1%) (Wardle, 2007). In Turkey, one study found a 2.9% GD prevalence among adults (Uygur, 2022), while a high school-based study reported gambling experience in 68.0% of males and 37.7% of females (Delice, 2017). Across contexts, men are generally at higher risk, and earlier initiation of gambling is consistently associated with more severe problems in adulthood (Australian Productivity Commission, 1999; Kessler et al., 2008).
Demographic variables such as gender, age, and socioeconomic status (SES) have been repeatedly linked to gambling behaviors. Males are more likely to initiate gambling earlier, engage in higher-risk and more frequent gambling, and report greater GD severity than females (Jimenez-Murcia et al., 2020; Wardle, 2007). While men often gamble for excitement, escape, or competition, women are more likely to use gambling as an emotion-focused coping mechanism (Arcan & Karancı, 2014; Potenza et al., 2001). Younger individuals and those from lower SES backgrounds also demonstrate increased vulnerability (Welte et al., 2008), suggesting that structural and psychosocial factors intersect in the development of gambling-related harm.
Object relations theory offers a psychodynamic framework for understanding the development of addictive behaviors such as GD. Rooted in the works of Klein (1952), Fairbairn (1946), and Winnicott (1965), the theory emphasizes the primacy of early interpersonal experiences—particularly the caregiver-infant bond—in shaping internal object representations. Unlike drive theory or ego psychology, object relations theory posits that relational needs, not biological instincts, drive behavior. Failures in early caregiving, such as unavailability or inconsistency, may lead to fragmented self-concepts and the internalization of punitive or absent object representations. In this view, addiction is understood as a compensatory strategy to manage internalized distress, wherein external objects like gambling substitute for unmet relational needs. Tools such as the Bell Object Relations and Reality Testing Inventory (BORRTI; Bell, 1995) have enabled the quantitative assessment of such intrapsychic structures through dimensions like Alienation, Egocentricity, and Social Incompetence.
Empirical research supports the association between disturbed object relations and addictive behaviors. Alienation, insecure attachment, and egocentric traits have been linked to increased relapse risk in substance use disorders (Khademi et al., 2020) and are also prominent in problem gambling. Adolescents with attachment anxiety and emotional regulation deficits are more likely to engage in addictive behavior (Estévez et al., 2017), while lower levels of cognitive empathy and emotional intelligence are associated with gambling problems (Parker et al., 2008; Zhou & Wu, 2024). During the COVID-19 pandemic, loneliness and social isolation were associated with increased gambling behavior, especially among first-time gamblers, who also reported elevated psychiatric symptoms (Forsström et al., 2022; Håkansson et al., 2020).
Loneliness, in particular, has emerged as a crucial psychological factor in the etiology of GD. From an object relations perspective, loneliness reflects early disruptions in attachment and internal object constellations, which can lead to chronic social disconnection and emotional dysregulation in adulthood (Ogden, 1989). Several studies have emphasized the mediating role of loneliness in the link between disturbed object relations and behavioral addictions (Trevorrow & Moore, 1998). Thus, loneliness may not only be a symptom but also a mechanism that amplifies vulnerability to gambling as a maladaptive coping strategy.
Furthermore, GD is associated with substantial impairments in quality of life across psychological, social, and economic domains. Affected individuals often experience elevated levels of depression, anxiety, and suicidality (Petry, 2005), alongside interpersonal disruptions such as family conflict, divorce, and social withdrawal. Financial burdens from gambling-related debt frequently exacerbate stress and erode support systems (Bernhard, 2007), contributing to a downward spiral of psychological and relational deterioration.
Accordingly, the present study aims to examine the relationship between object relations and GD, focusing on the mediating role of loneliness, and further evaluating how these factors influence quality of life. Given the limited research specifically exploring the intersection of object relations theory and GD, this study seeks to contribute to the theoretical understanding and provide implications for clinical and preventive interventions.
Methods
This study employed a cross-sectional and correlational research design based on the structural equation modeling (SEM) framework. The primary objective was to examine the direct and indirect relationships between object relations, loneliness, reality testing, gambling disorder (GD), and quality of life.
Quantitative data were collected through online self-report measures. The sample consisted of 443 adults residing in Turkey who volunteered to participate in the study. Participants were recruited through social media platforms and online forums. Inclusion criteria required participants to be over 18 years old and fluent in Turkish. Exclusion criteria included having a self-reported diagnosis of severe psychiatric disorders (e.g., schizophrenia, bipolar disorder) or cognitive impairments that would hinder survey comprehension. The final sample included 235 individuals who reported engaging in gambling at least once in the past year, and others who had not.
Demographically, 60.5% of the participants were male, and the average age was 30.41 (SD = 10.2). Most participants had a university-level education (68.6%) and lived in urban areas (74.2%) (Table 1).
| Table 1. Socio-demographic frequencies of the participations | |||||
| Category |
|
|
|
|
|
| Age Group | |||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
| Sex | |||||
|
|
|
|
|||
|
|
|
|
|||
| Education Level | |||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Employment status | |||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Monthly Income (Turkish Lira; TL) | |||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
| Monthly Gambling Expenditure (TL) | |||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Informed Consent and Measures
All participants provided informed consent prior to their participation in the study. They were informed about the aim of the research, the voluntary nature of their involvement, and their right to withdraw at any stage without any negative consequences. The study strictly adhered to ethical research principles, ensuring the anonymity and confidentiality of participant data throughout the research process.
Personal Information Form
A Personal Information Form was developed to gather participants’ sociodemographic and gambling-related background information. This included variables such as age, gender, education level, employment status, and monthly income. Additionally, participants were asked specific questions to assess gambling behaviors, including “At what age did you first gamble?” and “How much money do you spend monthly on gambling (Turkish Lira; TL)?”
South Oaks Gambling Screen (SOGS)
To assess gambling-related problems, the South Oaks Gambling Screen (SOGS), developed by Lesieur and Blume (1987), was used. This 20-item instrument evaluates the psychological, social, and economic effects of gambling behavior, with binary “Yes” or “No” responses. The original version demonstrated strong reliability, with a test-retest correlation of 0.95 and internal consistency of α = .86. The Turkish adaptation by Duvarcı and Varan (2001) modified the scale by removing three items irrelevant to Turkish culture and adding two culturally appropriate items, resulting in a 19-item version. A score of 8 or above indicates probable pathological gambling. In this study, the internal consistency coefficient was found to be α = .96, indicating excellent reliability.
Bell Object Relations and Reality Testing Inventory (BORRTI)
The BORRTI, developed by Bell (1995), is a 90-item instrument measuring both object relations and reality testing capacities through “True” or “False” responses. Object relations subscales include Alienation, Insecure Attachment, Egocentricity, and Social Incompetence, while reality testing includes Reality Distortion, Uncertainty of Perception, and Hallucinations and Delusions. The Turkish adaptation by Uluç et al. (2015) reported acceptable internal consistency coefficients (α = .70–.80). In the present study, Cronbach’s alpha values ranged from .80 to .91 across subscales, indicating strong reliability.
UCLA Loneliness Scale
Loneliness levels were measured using the UCLA Loneliness Scale (Russell et al., 1978), which includes 20 items scored on a 4-point Likert scale. Higher scores indicate greater perceived loneliness. The original internal consistency was α = .96, with test-retest reliability of .73. The Turkish version by Demir (1989) demonstrated high reliability (α = .96; test-retest = .94). In the current study, Cronbach’s alpha was calculated as .80.
World Health Organization Quality of Life Scale – Short Form (WHOQOL-BREF)
Participants’ quality of life was assessed using the WHOQOL-BREF (The Whoqol Group, 1998), a 26-item measure covering four domains: Physical Health, Psychological Health, Social Relationships, and Environment. Items are rated on a 5-point Likert scale reflecting the previous two weeks. Eser et al. (1999) adapted the Turkish version, reporting internal consistency coefficients of α = .83 for Physical Health, .66 for Psychological Health, .53 for Social Relationships, and .73 for Environment. In this study, the total reliability of the scale was α = .96, with subscale alphas ranging from .83 to .92, demonstrating strong psychometric properties.
Data Collection
Ethical approval for this study was granted by the Ethics Committee of the affiliated institution. Afterwards, participants voluntarily completed an online survey as part of the data collection process. A mixed-method sampling strategy was utilized to ensure a representative sample. Initially, snowball sampling was used to collect data from a general population by connecting with individuals in the researchers’ networks and expanding through their social circles.
Purposive sampling was later adopted to specifically target individuals predisposed to gambling behaviors. This involved targeting groups and platforms (e.g., relevant social media communities and online forums) where gambling behaviors were prevalent. Online data collection methods enabled access to individuals from diverse socioeconomic and demographic backgrounds. The sampling methods aimed to enhance both internal and external validity.
Analysis
The data collection process was completed between April 2024 and December 2024. Data from participants were digitized, and statistical analyses were conducted. Responses from five participants were excluded for inconsistency (e.g., entering an 11-digit number for the question, “What is the highest amount of money you have spent on gambling in a day?”) or for being under 18 years old.
Descriptive statistics and correlational analyses were conducted using IBM SPSS Statistics (Version 28). Frequency analysis was conducted to examine data distribution, and the Skewness and Kurtosis method was used to test normality. As variables followed a normal distribution, parametric tests were applied. Pearson correlation analysis was used to assess relationships between continuous variables. Independent samples t-tests were conducted to compare gamblers and non-gamblers.
To classify participants based on gambling behavior, the question “How much money do you spend monthly on gambling/betting/games of chance (in Turkish Lira; TL)?” was used. Participants spending 1 TL or more monthly were classified as ‘gamblers’ (n = 235), while those spending less than 1 TL or none were labeled ‘non-gamblers’.
The hypothesized model was tested using structural equation modeling (SEM) in AMOS 26. Goodness-of-fit indices, including chi-square (χ²), comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR), were used to evaluate how well the theoretical model fit the data.
Results
Gambling participation frequencies were analyzed for the total sample (N = 443) and for those who reported spending at least 1 TL monthly on gambling (n = 235). Participation rates were classified as “never,” “less than once per week,” and “once per week or more,” with the latter two combined to calculate overall participation.
The analysis (Table 2) indicated that scratch cards exhibited the highest participation rates across both groups. Scratch cards had the highest participation (61.2% overall; 86.4% among gamblers), followed by numeric lottery (81.3%) and national lottery (76.2%) in the gambling group. Card games for money and online betting were also common (74.5% and 69.4% among gamblers; 43.1% and 39.5% overall, respectively). Dice games (15.2% among gamblers) and casino games (44.2% among gamblers) had the lowest rates. These findings suggest that lottery-based activities were the most preferred forms of gambling.
| Table 2. Distribution of all participants and gamblers by types of gambling | ||||
|
|
|
|||
| Gambling Types |
|
|
|
|
| Betting |
|
|
|
|
| Online Roulette 21 |
|
|
|
|
| Other Types of Gambling (e.g., tennis) |
|
|
|
|
| Numerical Lottery |
|
|
|
|
| Scratch Cards |
|
|
|
|
| National Lottery |
|
|
|
|
| Stock Market Trading |
|
|
|
|
| Casino Games |
|
|
|
|
| Skill-Based Games for Money (e.g., billiards) |
|
|
|
|
| Online Betting |
|
|
|
|
| Card Games for Money (e.g., poker) |
|
|
|
|
| Rummy for Money |
|
|
|
|
| Dice Games for Money (e.g., craps) |
|
|
|
|
| Sports Lottery/Numerical Lottery |
|
|
|
|
Pearson correlation analysis (Table 3) examined the associations between gambling behaviors and variables such as age, income, age of first gambling, monthly gambling expenditure, and the expenditure/income ratio. SOGS scores were negatively but non-significantly related to income (r = −.09, p > .05), while a significant negative correlation was found with age of first gambling (r = −.11, p ≤ .05), indicating greater problem severity among early starters. SOGS scores showed significant positive correlations with monthly gambling expenditure (r = .39, p < .001) and the highest amount gambled in a day (r = .42, p < .001), suggesting that higher spending is linked to greater gambling problems. SOGS scores and daily maximum gambling were also negatively associated with age (r = −.11 and −.12, respectively; p < .05), indicating higher risk among younger individuals.
| Table 3. Correlation findings related to gambling behavior | ||||||
|
|
|
|
|
|
|
|
| 1. SOGS | ||||||
| 2. Age |
|
|||||
| 3. Monthly Income (Turkish Lira; TL) |
|
|
||||
| 4. Monthly Gambling Expenditure / Monthly Income |
|
|
|
|||
| 5. Age of First Time Gambling (onset) |
|
|
|
|
||
| 6. Monthly Gambling Expenditure (TL) |
|
|
|
|
|
|
| 7. Highest Amount Spent on Gambling in a Day (TL) |
|
|
|
|
|
|
| SOKTT: South Oaks Kumar Tarama Testi * p < .05, p < .01, ***p < .001; N = 443 | ||||||
A significant negative correlation was found between monthly income and age of first gambling (r = −.15, p < .01), suggesting that lower-income individuals began gambling earlier. Monthly income showed no significant relationship with average gambling expenditure (r = −.05, p > .05) or the highest single-day wager (r = .04, p > .05). A significant positive correlation was observed between the gambling expenditure/income ratio and SOGS scores (r = .30, p < .001), indicating greater problem severity among those spending a larger share of their income. Earlier gambling initiation was associated with higher monthly expenditure (r = −.14, p < .01), but not with the single-day maximum (r = −.04, p > .05). Lastly, monthly gambling expenditure was positively related to the highest amount gambled in a day (r = .32, p < .001).
To examine gender differences in gambling behaviors, Independent Samples t-Tests were conducted (see Table 4). The analysis revealed a significant difference in SOGS total scores between females (M = .75) and males (M = 7.02) (t = −11.59, p < .001), demonstrating that males exhibited markedly higher scores for problematic gambling behaviors than females.
| *p<.001 | ||||||
| Table 4. Comparison of variables by sex | ||||||
| Variable | Sex |
|
|
|
|
|
| SOGS | Female |
|
|
|
|
|
| Male |
|
|
|
|||
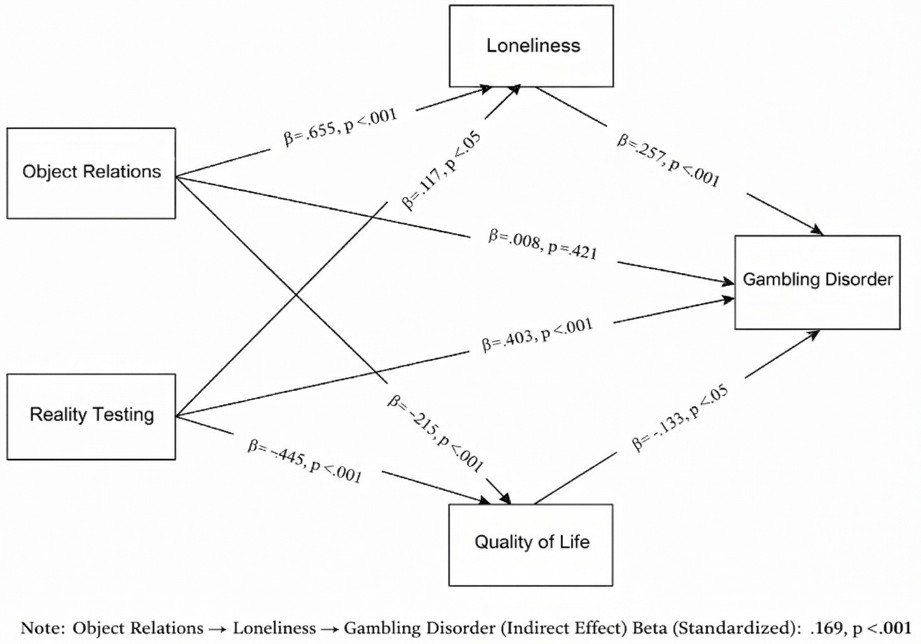
A Structural Equation Model (SEM) was employed to examine how Object Relations and Reality Testing affect Gambling Disorder (GD), both directly and indirectly, with Loneliness as a mediating variable. In the model, Object Relations and Reality Testing were specified as independent variables, while Loneliness and GD served as mediators and Quality of Life was the final outcome variable. The results indicated that Object Relations did not have a significant direct effect on GD (β = 0.008, p = .421), whereas Reality Testing showed a strong and significant direct effect on GD (β = 0.403, p < .001), suggesting that distortions in reality perception are closely linked to gambling severity.
Both Object Relations and Reality Testing significantly predicted Loneliness (β = 0.655, p < .001; β = 0.117, p = .042, respectively), and Loneliness, in turn, had a significant direct effect on GD (β = 0.257, p < .001). These findings suggest that impaired early relational patterns and reality distortions increase feelings of loneliness, which contributes to greater gambling problems. Additionally, indirect paths were confirmed: Object Relations had a significant indirect effect on GD through Loneliness (β = 0.168, p < .001), and Reality Testing also had a smaller but significant indirect effect via Loneliness (β = 0.030, p = .041). Regarding Quality of Life, both Object Relations (β = −.215, p < .001) and Reality Testing (β = −.445, p < .001) had significant negative effects. The model explained 41% of the variance in GD (R² = 0.410), 57% of the variance in Loneliness (R² = 0.575), and 53% of the variance in Quality of Life (R² = 0.533).
The model fit indices demonstrated the theoretical framework’s validity: χ² (14) = 28.12, p = 0.065; RMSEA = 0.029 (90% CI: 0.017–0.042); CFI = 0.990; TLI = 0.987; GFI = 0.980; AGFI = 0.970 (see Table 5). These values indicate excellent model fit and alignment with recommended thresholds (Tabachnick & Fidell, 2007). Figure 1 illustrates the structural relationships and standardized path coefficients.
| Table 5. Fit indices for the structural equation model | ||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Discussion
This study provides valuable findings concerning the associations between object relations, loneliness, and gambling disorder (GD), particularly highlighting the mediating role of loneliness and the detrimental impact of GD on quality of life. The results of the correlational analyses and structural equation modeling confirm most of the hypotheses and contribute to the theoretical and clinical understanding of GD.
The findings indicate that lottery-based gambling activities, such as scratch cards, numerical lottery, and national lottery, were the most frequently preferred types among both the general sample and individuals who gamble regularly. This may be attributed to their accessibility, perceived legality, and low entry cost. The high prevalence of scratch cards aligns with prior research suggesting that instant-win games appeal more strongly to habitual gamblers. Among individuals classified as gamblers, participation rates in certain gambling types—particularly those involving higher risk and potential illegality—were markedly higher than in the general sample, with notable increases observed in online betting, card games for money, and casino games, all of which may involve unregulated or illegal platforms within the Turkish context. The sharp contrast between the overall sample and the gambling subgroup in these categories suggests that frequent gamblers are more likely to engage in high-risk, fast-reward gambling behaviors. These activities are often associated with higher financial stakes, reduced perceived control, and increased cognitive distortions, which are known to exacerbate gambling-related harm. The elevated rates of participation in digital or informal gambling environments further imply a shift toward more persistent and less socially visible gambling patterns among this group, highlighting the importance of addressing risk propensity and regulatory gaps in intervention strategies.
A primary finding of the study was the significant negative correlation between age of first gambling and the total score on the South Oaks Gambling Screen (SOGS). This result is consistent with the literature indicating that individuals who start gambling at an earlier age are at heightened risk of developing more severe gambling problems later in life (Jimenez-Murcia et al., 2020; Wardle, 2007). Early onset of gambling appears to be associated with impulsivity, risk-taking tendencies, and a longer exposure to gambling-related reinforcement patterns. This finding underscores the need for preventive interventions during adolescence, a critical developmental period for shaping attitudes toward risk and behavioral regulation.
Another key finding was the significant positive relationship between the severity of GD and both monthly gambling expenditure and the highest amount of money gambled in a single day. These results are consistent with prior research suggesting that financial investment is closely linked with the intensity of gambling behavior (Bernhard, 2007). Interestingly, monthly income alone did not significantly predict gambling severity, indicating that problematic gambling behaviors may cut across different socioeconomic strata. A particularly noteworthy finding was that the ratio of monthly gambling expenditure to monthly income had a strong positive association with GD severity. This suggests that the proportion of income allocated to gambling—rather than absolute income—serves as a more accurate indicator of risk. This supports the view that perceived financial strain and over-commitment to gambling are stronger predictors of harm than income level per se (Blanco et al., 2015; Hodgins & Stevens, 2021).
The study also revealed findings regarding gender differences. Male participants were more likely to gamble, initiated gambling at earlier ages, and engaged in illegal forms of gambling behavior, consistent with both international and Turkish studies (Arcan & Karancı, 2014; Blanco, 2016; Griffiths & Wood, 2000; Uygur, 2022). These findings support the assertion that GD is strongly gendered in nature, with men overrepresented in clinical and community samples of gamblers. Moreover, gender differences extended to psychological motivations for gambling: men tended to gamble for excitement, status, or competitiveness—traits typically associated with externalizing tendencies—whereas women more often gambled in response to loneliness, stress, or emotional dysregulation (Dowling et al., 2021; Grant et al., 2007). These findings have implications for gender-sensitive prevention and treatment strategies, calling for adapted approaches that address impulsivity and loss-chasing in men, and emotional regulation and trauma in women.
The structural model offered further insights by identifying a significant indirect pathway from object relations to GD via loneliness. Specifically, object relations did not directly predict gambling severity, but dysfunctional object relations—such as feelings of alienation, egocentricity, and social ineffectiveness—contributed to increased levels of loneliness, which in turn predicted increased gambling behavior. This finding aligns with psychodynamic theories (e.g., Fairbairn, Winnicott) and empirical research emphasizing the role of early relational disruptions in shaping adult psychopathology. In the context of GD, this suggests that impaired internalized representations of others and difficulties in forming secure attachments may lead to social withdrawal and compensatory behaviors such as gambling.
Another significant finding was the direct effect of reality evaluation on GD. Individuals who exhibited distorted perceptions of reality—such as magical thinking, illusion of control, or cognitive misinterpretations—were more likely to report severe gambling symptoms. This result is supported by clinical and neurobiological studies (e.g., Corbeil et al., 2024; van Holst et al., 2012) demonstrating that distorted cognitive processes are core mechanisms maintaining gambling behavior. Subscales such as “Distortion of Reality” and “Hallucinations/Delusions” may reflect the underlying beliefs and perceptual biases that reinforce maladaptive decision-making in gambling contexts.
The study also revealed that both object relations and reality evaluation had direct and negative effects on quality of life, independently of gambling severity. Poor object relations predicted lower psychological and social well-being, while compromised reality testing was associated with greater emotional distress and impaired functioning. Most prominently, GD itself demonstrated a strong and negative association with all domains of quality of life—physical, psychological, social, and environmental—validating findings from prior research (Bonfils et al., 2022; The Whoqol Group, 1998).
These findings collectively underscore the importance of comprehensive treatment strategies for GD. Interventions must address not only the behavioral symptoms but also the underlying emotional, psychodynamic, cognitive, and relational difficulties. Cognitive-behavioral therapy (CBT), trauma-informed care, and relationally focused approaches such as schema therapy or psychodynamic psychotherapy may be particularly effective. Moreover, the mediating role of loneliness points to the necessity of rebuilding social connectedness and addressing interpersonal functioning as part of therapeutic goals.
The study’s integration of intrapsychic, interpersonal, and cognitive predictors of GD provides empirical support for the Pathways Model (Blaszczynski & Nower, 2002), which distinguishes between behaviorally conditioned, emotionally vulnerable, and antisocial-impulsive pathways to gambling. The findings especially align with the emotionally vulnerable pathway, characterized by early attachment issues, loneliness, and emotional dysregulation.
Limitations and Directions/Suggestions for Future Research
Limitations include the cross-sectional design, which excludes causal interpretations; reliance on self-report measures, which may be biased due to social desirability effects, recall bias, or variability in self-awareness. This limitation is particularly relevant for behaviors such as gambling, which may be socially stigmatized and thus underreported or distorted. Additionally, the sample consisted solely of participants from Turkey and was recruited online, limiting the cultural generalizability of the findings. Individuals with limited internet access or from socioeconomically disadvantaged, older, or less-educated groups may have been underrepresented in the model. Furthermore, the use of mixed sampling methods, including snowball and purposive sampling, may limit the representativeness of the sample and should be considered when interpreting the generalizability of the findings.
Future research should employ longitudinal designs to examine causal directions among variables, incorporate clinical populations to enhance generalizability, and explore additional psychological factors such as trauma, impulsivity, and emotion regulation. Cross-cultural comparisons could also offer insight into the sociocultural dynamics influencing GD. Mixed-methods studies integrating qualitative interviews would deepen the understanding of subjective experiences related to object relations, loneliness, and reality perception.
In sum, this study highlights that GD is not merely a behavioral issue but a complex psychosocial syndrome embedded in impaired object relations, distorted cognition, and emotional disconnection. Interventions should therefore be multidimensional, integrating psychodynamic, cognitive-behavioral, and systemic approaches to address both symptoms and underlying mechanisms. Public health policies should also prioritize community-level strategies that mitigate social isolation and promote psychological resilience, especially in high-risk populations.
Ethical approval
This study was approved by the Istanbul Arel University Graduate Education Institute Ethical Committee (Date: March 22, 2024, Decision/Protocol No: E-69396709-050.04-568581 2024/07). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425596
- Arcan, K., & Karancı, A. (2014). Adaptation, validity, and reliability study of the five-factor gambling motives scale. Anatolian Journal of Psychiatry, 15(3), 248. https://doi.org/10.5455/apd.48431
- Australian Productivity Commission. (1999). Australia’s gambling industries: Fact sheet: The costs and benefits of gambling. Productivity Commission.
- Bell, M. D. (1995). Bell object relations and reality testing inventory manual. Western Psychological Services.
- Bernhard, B. J. (2007). The voices of vices: Sociological perspectives on the pathological gambling entry in the diagnostic and statistical manual of mental disorders. American Behavioral Scientist, 51(1), 8-32. https://doi.org/10.1177/0002764207304869
- Blanco, C., Hanania, J., Petry, N. M., Wall, M. M., Wang, S., Jin, C. J., & Kendler, K. S. (2015). Towards a comprehensive developmental model of pathological gambling. Addiction, 110(8), 1340-1351. https://doi.org/10.1111/add.12946
- Blanco, R. M. (2016). Experiential avoidance, mindfulness, and values clarification as moderaters of the association between impulsivity and gambling behavior (Publication No. 10246559) [Doctoral dissertation, Illinois Institute of Technology]. ProQuest Dissertations & Theses Global.
- Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97(5), 487-499. https://doi.org/10.1046/j.1360-0443.2002.00015.x
- Bonfils, N. A., Aubin, H. J., Grall-Bronnec, M., Caillon, J., Perney, P., Limosin, F., & Luquiens, A. (2022). Development and psychometric properties of a new patient-reported outcome instrument of health-related quality of life specific to patients with gambling disorder: The gambling quality of life scale (GQoLS). International Journal of Environmental Research and Public Health, 19(17), 10806. https://doi.org/10.3390/ijerph191710806
- Corbeil, O., Anderson, É., Béchard, L., Desmeules, C., Huot‐Lavoie, M., Bachand, L., Brodeur, S., Carmichael, P., Jacques, C., Solmi, M., Giroux, I., Dorval, M., Demers, M., & Roy, M. (2024). Problem gambling in psychotic disorders: A systematic review and meta‐analysis of prevalence. Acta Psychiatrica Scandinavica, 149(6), 445-457. https://doi.org/10.1111/acps.13686
- Delice, Y. (2017). Lise düzeyindeki ergenlerin kumar oynamaları ile riskli davranışları arasındaki ilişkiler (Thesis No. 469373) [Master’s thesis, Maltepe University]. Council of Higher Education National Thesis Center.
- Demir, A. G. (1989). UCLA yalnızlık ölçeğinin geçerlik ve güvenirliği. Psikoloji Dergisi, 7(23), 14-18. https://psikolog.org.tr/tr/yayinlar/dergiler/1031828/tpd1300443319890000m000359.pdf
- Dowling, N. A., Youssef, G. J., Greenwood, C., Merkouris, S. S., Suomi, A., & Room, R. (2021). The development of empirically derived Australian low-risk gambling limits. Journal of Clinical Medicine, 10(2), 167. https://doi.org/10.3390/jcm10020167
- Duvarcı, I., & Varan, A. (2001). Reliability and validity study of the Turkish form of the South Oaks gambling screen. Turk Psikiyatri Dergisi, 12(1), 34-45. https://www.turkpsikiyatri.com/PDF/C12S1/southOaksKumar.pdf
- Eser, E., Fidaner, H., Fidaner, C., Eser, S. Y., Elbi, H., & Göker, E. (1999). WHOQOL-100 ve WHOQOL-BREF’in psikometrik özellikleri. Psikiyatri Psikoloji Psikofarmakoloji (3P) Dergisi, 7(Suppl 2), 23-40.
- Estévez, A., Jáuregui, P., Sánchez-Marcos, I., López-González, H., & Griffiths, M. D. (2017). Attachment and emotion regulation in substance addictions and behavioral addictions. Journal of Behavioral Addictions, 6(4), 534-544. https://doi.org/10.1556/2006.6.2017.086
- Fairbairn, W. R. D. (1946). Object-relationships and dynamic structure. The International Journal of Psychoanalysis, 27, 30-37.
- Ferentzy, P., & Turner, N. E. (2013). The history of problem gambling: Temperance, substance abuse, medicine, and metaphors. Springer. https://doi.org/10.1007/978-1-4614-6699-4
- Forsström, D., Lindner, P., Månsson, K. N. T., Ojala, O., Hedman-Lagerlöf, M., El Alaoui, S., Rozental, A., Lundin, J., Jangard, S., Shahnavaz, S., Sörman, K., Lundgren, T., & Jayaram-Lindström, N. (2022). Isolation and worry in relation to gambling and onset of gambling among psychiatry patients during the COVID-19 pandemic: A mediation study. Frontiers in Psychology, 13, 1045709. https://doi.org/10.3389/fpsyg.2022.1045709
- Gabellini, E., Lucchini, F., & Gattoni, M. E. (2022). Prevalence of problem gambling: A meta-analysis of Recent Empirical Research (2016-2022). Journal of Gambling Studies, 39(3), 1027-1057. https://doi.org/10.1007/s10899-022-10180-0
- Grant, J. E., Williams, K. A., & Potenza, M. N. (2007). Impulse-control disorders in adolescent psychiatric inpatients: Co-occurring disorders and sex differences. Journal of Clinical Psychiatry, 68(10), 1584. https://doi.org/10.4088/JCP.v68n1018
- Griffiths, M., & Wood, R. T. (2000). Risk factors in adolescence: The case of gambling, videogame playing, and the internet. Journal of Gambling Studies, 16(2), 199-225. https://doi.org/10.1023/A
- Håkansson, A., Fernández-Aranda, F., Menchón, J. M., Potenza, M. N., & Jiménez-Murcia, S. (2020). Gambling during the COVID-19 crisis - A cause for concern. Journal of Addiction Medicine, 14(4), e10-e12. https://doi.org/10.1097/ADM.0000000000000690
- Hodgins, D. C., & Stevens, R. M. (2021). The impact of COVID-19 on gambling and gambling disorder: emerging data. Current Opinion in Psychiatry, 34(4), 332-343. https://doi.org/10.1097/YCO.0000000000000709
- Jimenez-Murcia, S., Granero, R., Giménez, M., Del Pino-Gutiérrez, A., Mestre-Bach, G., Mena-Moreno, T., Moragas, L., Baño, M., Sánchez-González, J., De Gracia, M., Baenas-Soto, I., Contaldo, S. F., Valenciano-Mendoza, E., Mora-Maltas, B., López-González, H., Menchón, J. M., & Fernández-Aranda, F. (2020). Contribution of sex on the underlying mechanism of the gambling disorder severity. Scientific Reports, 10(1), 18722. https://doi.org/10.1038/s41598-020-73806-6
- Kessler, R. C., Hwang, I., LaBrie, R., Petukhova, M., Sampson, N. A., Winters, K. C., & Shaffer, H. J. (2008). DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychological Medicine, 38(9), 1351-1360. https://doi.org/10.1017/S0033291708002900
- Khademi, M. J., Monirpoor, N., Ebrahimi, Z., & Rashedi, V. (2020). Object relations and vulnerability to substance abuse relapse among substance abusers visiting narcotics anonymous centers in Qom City, 2018.
- Klein, M. (1952). The origins of transference. International Journal of Psychoanalysis, 33(4), 433-438.
- Lesieur, H. R., & Blume, S. B. (1987). The south oaks gambling screen: A new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144(9), 1184-1188. https://doi.org/10.1176/ajp.144.9.1184
- Ogden, T. A. (1989). On the concept of an autistic-contiguous position. The International Journal of Psycho-Analysis, 70, 127-140. https://pubmed.ncbi.nlm.nih.gov/2535621/
- Parker, J. D. A., Taylor, R. N., Eastabrook, J. M., Schell, S. L., & Wood, L. M. (2008). Problem gambling in adolescence: Relationships with internet misuse, gaming abuse and emotional intelligence. Personality and Individual Differences, 45(2), 174-180. https://doi.org/10.1016/j.paid.2008.03.018
- Petry, N. M. (2005). Pathological gambling: Etiology, comorbidity, and treatment. American Psychological Association. https://doi.org/10.1037/10894-000
- Potenza, M. N., Steinberg, M. A., McLaughlin, S. D., Wu, R., Rounsaville, B. J., & O’Malley, S. S. (2001). Gender-related differences in the characteristics of problem gamblers using a gambling helpline. American Journal of Psychiatry, 158(9), 1500-1505. https://doi.org/10.1176/appi.ajp.158.9.1500
- Russell, D., Peplau, L. A., & Ferguson, M. L. (1978). Developing a measure of loneliness. Journal of Personality Assessment, 42(3), 290-294. https://doi.org/10.1207/s15327752jpa4203_11
- Tabachnick, B. G., & Fidell, L. S. (2007). Experimental designs using ANOVA (Vol. 724). Thomson/Brooks/Cole.
- The Whoqol Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551-558. https://doi.org/10.1017/s0033291798006667
- Trevorrow, K., & Moore, S. (1998). The association between loneliness, social isolation and women’s electronic gaming machine gambling. Journal of Gambling Studies, 14(3), 263-284. https://doi.org/10.1023/A
- Uluç, S., Tüzün, Z., Haselden, M., & Erbaş, S. P. (2015). Bell Nesne İlişkileri ve Gerçeği Değerlendirme Ölçeği’nin Türkçe’ye uyarlama çalışması. Klinik Psikiyatri Dergisi, 18(4), 112-123.
- Uygur, A. B. (2022). Kumar oynama bozukluğunun davranişsal inhibisyon-aktivasyon sistemleri ve sosyodemografik etkenler ile ilişkisi. Kahramanmaraş Sütçü İmam Üniversitesi Tıp Fakültesi Dergisi, 17(1), 36-45. https://doi.org/10.17517/ksutfd.862992
- van Holst, R. J., Veltman, D. J., Büchel, C., van den Brink, W., & Goudriaan, A. E. (2012). Distorted expectancy coding in problem gambling: Is the addictive in the anticipation? Biological Psychiatry, 71(8), 741-748. https://doi.org/10.1016/j.biopsych.2011.12.030
- Wardle, H. (2007). British gambling prevalence survey 2007. The Stationery Office.
- Welte, J. W., Barnes, G. M., Tidwell, M.-C. O., & Hoffman, J. H. (2008). The prevalence of problem gambling among U.S. adolescents and young adults: Results from a national survey. Journal of Gambling Studies, 24(2), 119-133. https://doi.org/10.1007/s10899-007-9086-0
- Winnicott, D. W. (1965). A clinical study of the effect of a failure of the average expectable environment on a child’s mental functioning. The International Journal of Psycho-Analysis, 46, 81-87.
- Zhou, H., & Wu, A. M. S. (2024). The protective effects of cognitive empathy and emotional empathy on gambling disorder are mediated by risk aversion and responsible gambling attitude. BMC Psychiatry, 24(1), 63. https://doi.org/10.1186/s12888-024-05509-5
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.