Abstract
The tobacco epidemic is a public health threat, killing more than 8 million people annually. Liquorice is an herbal medicine that acts as a modulator of GABA receptors and may induce sedative and anxiolytic effects; thereby, it can support smoking cessation. This study aimed to assess the efficacy of liquorice root and sugarless chewing gum in smoking cessation using a randomized controlled trial design.
Smokers aged 18 to 74 years attending a tobacco cessation centre were recruited. A total of 116 smokers were recruited, and written informed consent was obtained. The level of tobacco dependence was assessed using Fagerstrom addiction score at baseline. Fifty-eight participants were allocated to the liquorice group (LG) and 58 to the chewing gum group (CG). Both groups received tobacco cessation counselling. The LG received liquorice root and CG received sugarless chewing gum for four weeks. Follow-up was conducted at 1, 2 and 3 months to evaluate self-reported continuous tobacco abstinence, relapse rate, Fagerstrom addiction scores and CO breath levels in both groups.
The present study demonstrated a significant reduction in smoking measures (self-reported continuous abstinence and carbon monoxide breath levels and Fagerstrom addiction scores) in the liquorice group compared with the chewing gum group. Self-reported continuous abstinence at 3 months was 72.4% and 60.3% in LG and CG, respectively. There was a statistically significant difference in the levels of exhaled CO reduction between LG and CG at 2 months (P=0.046) and 3 months (P=0.013)
In the current trial, liquorice root demonstrated superior efficacy over sugarless chewing gum as a substitute for a smoking form of tobacco.
Keywords: liquorice, chewing gum, smoking cessation, tobacco cessation
Main Points
- The study evaluates the effectiveness of liquorice root and sugarless chewing gum as adjuvant aids for smoking cessation in a randomized controlled trial among adult smokers.
- Liquorice root demonstrated a greater reduction in Fagerstrom nicotine dependence scores and exhaled carbon monoxide levels compared to sugarless chewing gum over a 3-month follow-up period.
- The self-reported continuous abstinence rate was higher in the liquorice group, indicating better smoking cessation outcomes, although not statistically significant.
- Liquorice root’s natural anxiolytic and oral gratification properties may contribute to its superior efficacy as a tobacco substitute.
- The findings support the use of liquorice root as a low-cost, culturally acceptable, and non-pharmacological intervention for tobacco cessation in resource-limited settings.
Introduction
Tobacco use remains one of the most pressing global public health concerns, contributing significantly to morbidity and mortality worldwide. According to the World Health Organization (2024), tobacco kills more than 8 million people annually, making it one of the leading preventable causes of death. In India, the burden of tobacco-related diseases is particularly high, necessitating effective cessation strategies. Recognizing this, the Dental Council of India in 2018 mandated the establishment of Tobacco Cessation Centres (TCCs) in all dental institutions, underscoring the role of oral healthcare professionals in tobacco control initiatives.
Apart from self-help strategies for quitting tobacco, various approaches have been suggested by the National Guidelines for Tobacco Cessation (Ministry of Health and Family Welfare, 2018), including pharmacological agents such as nicotine replacement therapies (NRTs) and non-nicotine-based medications such as bupropion SR and varenicline (U.S. Public Health Service, 2008). Non-pharmacological agents such as chewing gums have also been used as substitutes for cigarette smoking in dependent smokers to reduce cravings and help cope with withdrawal symptoms (Cohen et al., 1997). Various alternative therapies—including hypnosis, acupuncture, yoga therapy, dietary aids, and low-level laser therapy—have also been explored for smoking cessation (Naresh et al., 2016).
Despite the availability of numerous agents for tobacco cessation, quitting requires a high level of cooperation, motivation, and compliance among tobacco users. Moreover, some agents themselves are addictive, expensive, or associated with adverse effects. This underscores the importance of exploring traditional products as potential cessation aids, since they may be more effective in terms of having fewer side effects, lower addictive potential, and greater cost-effectiveness (Mitra et al., 2023).
One such traditional herbal medicine is liquorice (Glycyrrhiza glabra Linn.), which has long been valued in ethnopharmacology. Liquorice has been reported to exhibit anti-inflammatory, antibacterial, antifungal, antidiabetic, antiviral, anti-ulcer, anticarcinogenic, antimutagenic, antitussive, antioxidant, anxiolytic, skin-lightening, and antidiuretic properties (Damle, 2014). It has also been traditionally used as a natural sweetener due to its distinctive taste. The high phenolic content in ethanolic extracts of liquorice (Glycyrrhiza glabra L.) is largely responsible for its antioxidant and free radical scavenging activities. Liquorice extract (block, powder, or liquid) has even been incorporated into cigarettes, at levels of 1–4%, to harmonize smoke flavor, enhance moisture retention, and act as a surface-active agent for ingredient application (Carmines et al., 2005). Its antitussive and expectorant effects are beneficial in treating sore throat and cough among smokers. Moreover, liquorice is known to act as a modulator of GABAA receptors, thereby exerting sedative and anxiolytic effects, since gamma-aminobutyric acid (GABA) is the major inhibitory neurotransmitter in the central nervous system (Pastorino et al., 2018).
A review of the scientific literature reveals a paucity of studies on liquorice root as an adjuvant aid for tobacco cessation in humans. Thus, the present study was designed to assess the efficacy of liquorice root and sugarless chewing gum as adjuncts to smoking cessation counselling among patients visiting a Tobacco Cessation Counselling Centre, using a randomized controlled trial design. The research hypothesis was that there is a significant difference in smoking cessation rates between the liquorice group and the sugarless chewing gum group. The primary outcome of the trial was the self-reported quit rate at the 3-month follow-up in both groups, with a comparison of efficacy between the liquorice group (LG) and the chewing gum group (CG).
Methods
Study Setting
A 3–month, concurrent, parallel, randomized controlled trial was conducted at a tobacco cessation clinic. Ethical approval was taken from the institutional ethical review board before the initiation of the trial (IRB Reference number:1/IRB/2022). The study was registered in the Clinical Trial Registry.
Recruitment of the Participants
The general public was informed about the tobacco cessation intervention program through newspaper pamphlets and smoking cessation camps. Participants were also recruited from the outpatient department of the dental institution. The participants who fulfilled the following inclusion and exclusion criteria were included in the trial.
Inclusion criteria:
- Current smokers aged 18 years to 74 years
- Smokers motivated to quit smoking
- Smokers with a Fagerstrom nicotine dependence score of 5 or more (moderate-to-high dependence)
- Smokers who gave written informed consent.
Exclusion criteria:
- Physically and mentally challenged individuals
- Subjects under medications for all chronic non-communicable diseases
- Subjects currently undergoing tobacco cessation using NRT or antidepressants
- Subjects currently using any other substance of abuse
- Subjects diagnosed with oral cancer
Sample Size
The sample size was calculated using a pilot study. The sample size at a 95% confidence interval, 90% power, and 0.641 effect size was calculated to be 53 participants in each group. However, the sample size was increased to 58 per group after adjusting for 10% dropouts. Hence, the final sample size was 116 participants in total.
Randomization
Out of the total 168 interested participants screened over a period of 6 months (March 2023 to August 2023), 116 participants who met the inclusion and exclusion criteria were included in the study. Participants were randomly assigned to one of two intervention groups with a 1:1 allocation ratio. Randomization was done using a computer-generated random numbers list. Each participant was assigned a number using a random number sequence and received the corresponding intervention. It was an open labelled RCT and no blinding procedure was followed.
Intervention Groups
The intervention was given to the study participants for a period of 1 month, with follow-up of smoking status for 3 months.
Intervention for the Study Group [Liquorice Group- LG]
In the LG, participants received Tobacco Cessation Counselling. The study participants were provided with pre-cut liquorice root packaged in 1-week packets, in an air sealed bag, for 4 weeks. Participants were instructed to chew liquorice root (1 gram) for 10 – 20 minutes, 3 to 5 times per day depending on craving of smoking. Participants were instructed to chew the root fully, swallow the juices, and spit out the remaining liquorice root after 20 minutes. Participants were advised to report any adverse reaction immediately.
Intervention for the Control Group [Sugarless Chewing Gum Group - CG]
In the CG, participants received tobacco cessation counselling and sugarless chewing gum (Orbit) packaged in 1-week packets, in an air sealed bag, for 4 weeks. Participants were advised to chew the chewing gum for 10 – 20 minutes, 2 to 3 times per day depending on craving of smoking. Participants were instructed to chew and spit out the gum after 20 mins.
All participants were given standardized instructions on how to use the assigned product. To minimize potential bias, participants in both groups were informed only that the intervention they received may help reduce cravings and support smoking cessation. They were not specifically told whether the product was a conventional cessation aid or a natural product, thereby reducing the risk of expectancy or placebo effects influencing outcomes.
Outcome Assessment
Operational Definition
Current smokers - Current smokers are defined as adults who have smoked 100 cigarettes in their lifetime and who currently smoke cigarettes.
Continuous abstinence - Continuous abstinence is defined as the stoppage of use of any form of tobacco (not even a puff) for 30 days from the initial quit day.
Quit attempt – Attempt to quit tobacco usage for one complete day (24 hours) after a grace period of 7 days from the initial assessment.
Relapse –Relapse is defined as reverting back to smoking any time after the initial quit day.
Assessment Variables
At baseline the variables assessed for both groups:
- Sociodemographic data.
- Type of smoked tobacco, age of onset, average use per day, duration of usage.
- Assessment of Fagerstrom score for nicotine dependence.
- Self-reported quit – continuous abstinence, relapse
- Objective assessment - Breath analysis using a CO breath analyzer.
At 1-, 2- and 3- month follow-up, the following outcomes were assessed in both groups:
- Fagerstrom score for nicotine dependence.
- Self-reported quit - continuous abstinence, relapse.
- Objective assessment using a CO breath analyser, comparing LG and CG
Statistical Analysis
For maintaining the database, statistical analyses were conducted using IBM Statistical Package for the Social Sciences (SPSS) Version 21. Normality of the data was checked using the Kolmogorov-Smirnov test, and the data were found to be nonparametric. Descriptive analyses were performed for sociodemographic data. Intragroup comparison of CO breath levels and Fagerstrom addiction scores were conducted using the Friedman test. Intergroup comparisons of CO breath levels and Fagerstrom addiction scores were conducted using the Mann-Whitney test. Intergroup and intragroup comparisons of self-reported abstinence and relapse rates were conducted using the chi-square test.
Results
Study Participants
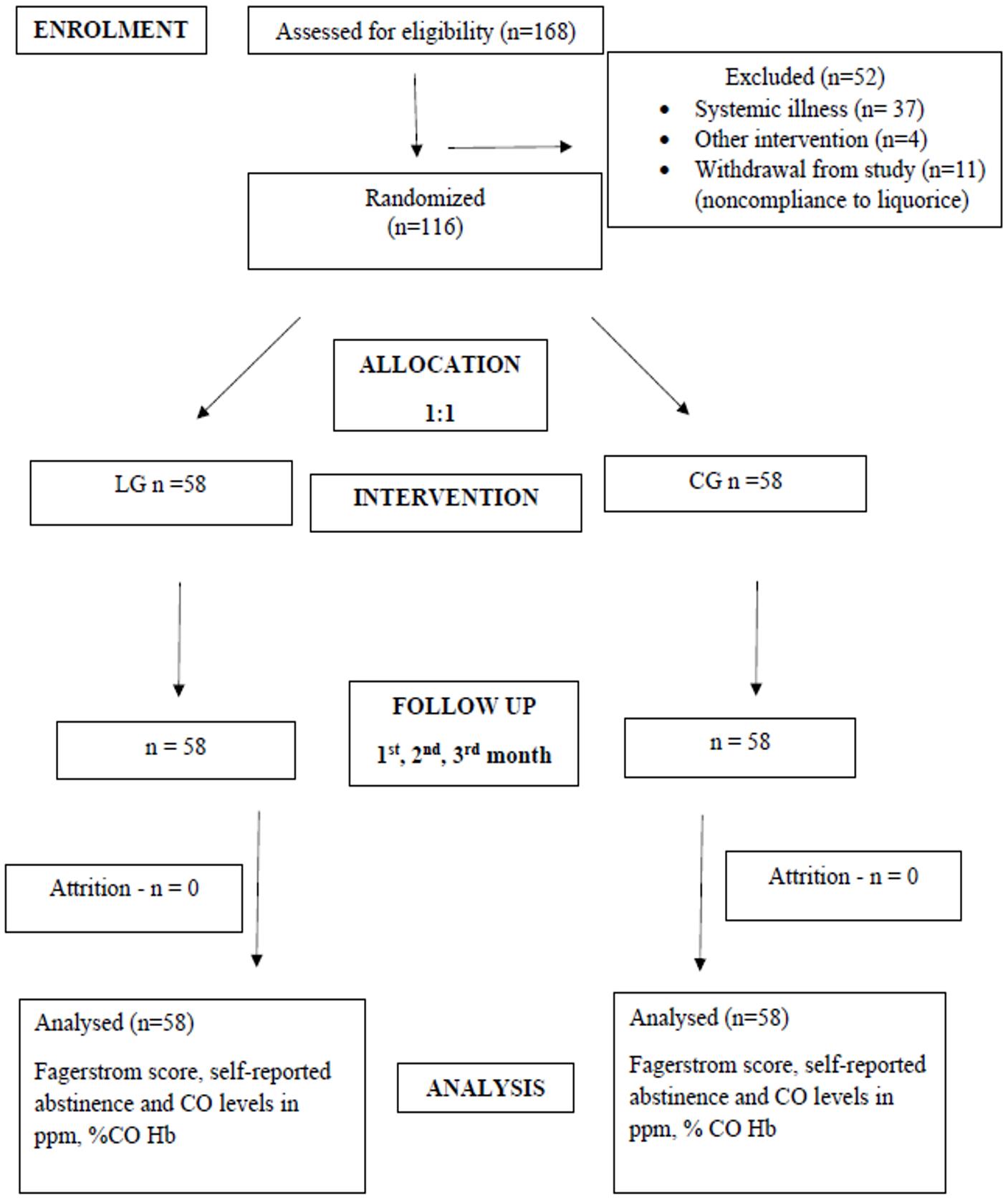
Of the 168 participants screened, 116 were included in the trial (58 in each group), and the sample size was maintained at 116 at the end of trial, with no loss to follow-up (Figure 1).
The age of study participants ranged from 24 to 59 years with a mean age of 46.02±12.88 years in the LG and 40.93±12.98 years in the CG. No females reported smoking status during the recruitment period, resulting in an all-male study participant cohort. Moreover, no major difference was observed in socioeconomic status between the LG and CG (Table 1).
| S.D. = standard deviation; LG = Liquorice Group; CG = Chewing gum Group. | |||
| Table 1. Sociodemographic characteristics | |||
| Variables |
|
|
|
| Age in years (Mean ± S.D.) |
|
|
|
| Gender n (%) | Male |
|
|
| Female |
|
|
|
| Socioeconomic status n (%) | Upper |
|
|
| Upper-Middle |
|
|
|
| Lower-Middle |
|
|
|
| Upper-Lower |
|
|
|
| Lower |
|
|
|
Baseline Analysis
At baseline, the average number of cigarettes/bidis smoked by study participants was 14.15±4.57, with 14.86±7.66 in LG and 14.42±8.52 in the CG. There was no statistically significant difference (p-value=0.824) between the mean number of cigarettes smoked in the LG and CG. Similarly, there was no statistically significant difference (p-value=0.250) between the mean number of years smoked (LG is 24.81±14.73 and CG is 22.26±12.75) between the groups (Table 2).
| aIndependent t test; bMann Whitney test; *Significant p-value <0.05. | |||
| Table 2. Baseline characteristics | |||
| Variables |
|
|
|
| Number of cigarettes/Bidi per day (Mean ± S.D.) |
|
|
|
| Number of years smoked (Mean ± S.D.) |
|
|
|
| Fagerstrom Addiction score (Mean ± S.D.) |
|
|
|
| CO level (ppm) (Mean ± S.D.) |
|
|
|
However, a statistically significant difference (p-value=0.035) was observed in the mean Fagerstrom addiction score at baseline (LG -5.90±2.13 and CG -5.12±1.98), with the LG having higher mean addiction scores. Likewise, a statistically significant difference (p-value=0.049) was observed in the CO levels between the LG and CG (LG- 21.72± 4.69 and CG- 20.17±7.35) with higher CO levels in the LG (Table 2).
Post – Intervention Outcome Analysis
Subjective Assessment at Baseline vs Post-Intervention
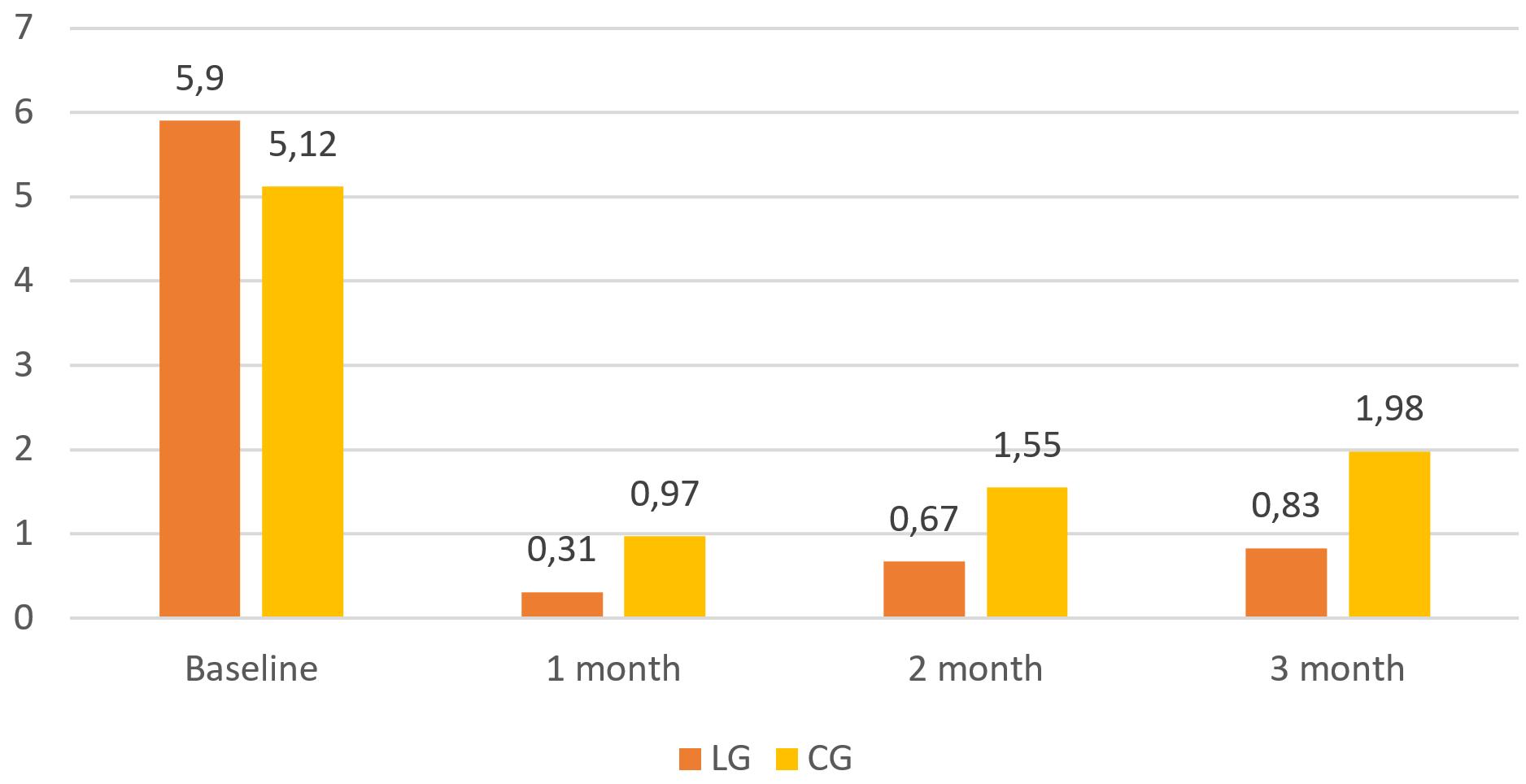
There was a significant reduction in smoking addiction scores during the 3-month follow-up in both the LG and CG (Table 3). However, the mean addiction scores were consistently lower in the LG compared to the CG (Figure 2).
| aFreidman test; *Significant P <0.05; ppm = parts per million. | ||||||
| Table 3. Comparison of Fagerstrom Addiction score and CO level in ppm and % CO Hb within LG and CG | ||||||
| Smoking status |
|
|
|
|
|
|
| CO level (ppm) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| CO level (%CO Hb) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Fagerstrom Addiction score |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective Assessment at Baseline vs Post-Intervention
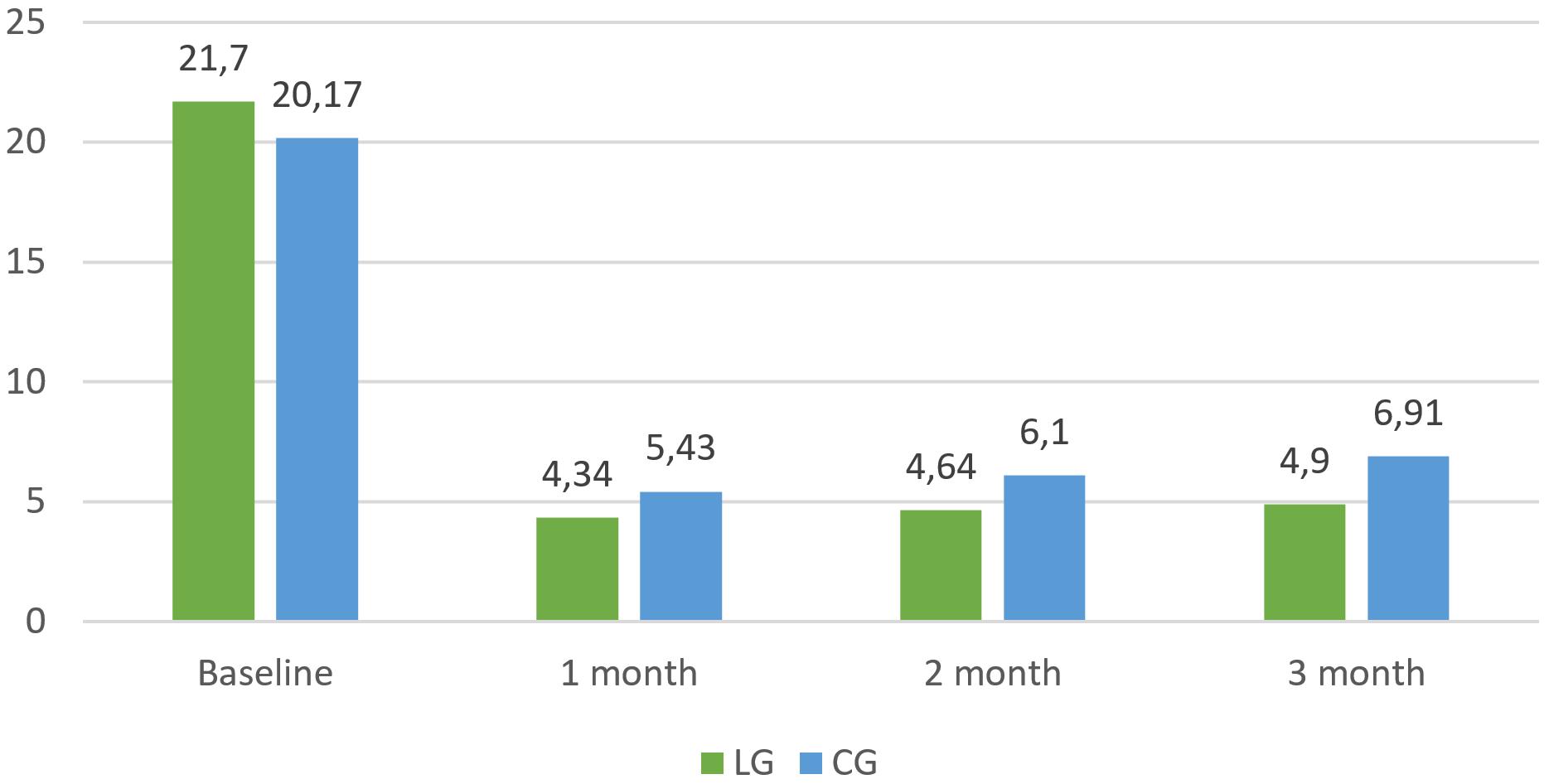
There was a significant reduction in scores of CO breath levels during the 3-month follow-up in both the LG and CG (Table 4). However, the mean CO breath levels were lower in the LG compared to the CG group, with a statistically significant difference between the LG and CG at the 2nd month and 3rd month of follow-up (Figure 3, Table 4).
| aMann whitney test; *Significant p-value <0.05; **Highly significant p-value <0.01. | ||||
| Table 4. Comparison of Fagerstrom Addiction score and CO in ppm and %CO Hb between LG and CG | ||||
| Smoking status |
|
|
|
|
| Carbon monoxide level (ppm) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Carbon monoxide level (%CO Hb) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Fagerstrom Addiction score |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subjective Assessment at 1st vs 2nd vs 3rd-Month Follow-Up
Intergroup comparison
Clinically, self-reported continuous abstinence was higher in the LG compared to the CG, although it lacked statistical significance. Relapse was lower in the LG compared to the CG; however, no statistically significant difference was seen between the two groups (Table 5).
| aChi square test; *Significant p-value <0.05. | ||||
| Table 5. Comparison of self–reported smoking status and relapse rate between LG and CG | ||||
| Smoking status |
|
|
|
|
| Self-reported abstinence rate |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Relapse rate |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Intragroup comparison
There was a statistically significant difference in self-reported continuous abstinence and relapse during the follow-up (i.e., 1st vs 2nd vs 3rd month) on analysis within the LG and CG, indicating that the intervention was effective in both the groups (Table 6).
| aChi square test; *Significant p-value <0.05. | ||||
| Table 6. Comparison of self-reported smoking status and relapse rate within LG and CG | ||||
| Smoking status |
|
|
|
|
| Self-reported abstinence rate |
|
|
|
|
|
|
|
|
|
|
| Relapse rate |
|
|
|
|
|
|
|
|
|
|
Discussion
According to the Global Adult Tobacco Survey conducted in 2016–2017, tobacco is consumed by 28.6% of the total population of India, of which smoking tobacco is consumed by 10.7% of the population (Ministry of Health and Family Welfare, 2017). Hence, there is a pressing demand for efficient tobacco cessation techniques to combat tobacco-related morbidity and mortality.
This study is the first of its kind to assess the use of liquorice root as an intervention agent to assist smoking cessation. There is also a paucity of research studying the efficacy of sugarless chewing gum as a substitute for a smoking form of tobacco. Therefore, the current study aimed to determine the efficacy of liquorice root and sugarless chewing gum as an adjunct to smoking cessation. The difference in recommended frequency between liquorice root (3–5 times/day) and chewing gum (2–3 times/day) was determined by the nature of the products. Liquorice root, being a natural product without standardized dosing guidelines, was advised more frequently to better replicate the hand-to-mouth action and oral gratification associated with smoking. In contrast, chewing gum is an established cessation aid with standard usage recommendations of 2–3 times daily. This rationale guided the frequency difference between the two interventions.
The information provided to participants at baseline can influence cessation outcomes through expectancy effects. In this study, efforts were made to provide neutral instructions, informing both groups that their assigned product may help in managing cravings, without highlighting liquorice as a natural aid or gum as a standard cessation product. This approach was intended to minimize placebo-related bias; however, the possibility of some expectancy effects cannot be completely excluded.
In the present study, we found that there was no significant difference in the continuous abstinence achieved at 3 months between the two intervention groups (p = .238). The effectiveness of interventions was, as expected, most evident during the intervention period and declined during the follow-up. Almost 35% of smokers were able to quit smoking at the end of three months.
The Fagerstrom Test for Nicotine Dependence (FTND) is a self-reported questionnaire that is easy to use and gives immediate feedback with good sensitivity and specificity to assess the nicotine dependence of smokers for clinical treatment and research (Heatherton et al., 1991). There was a statistically significant reduction in Fagerstrom addiction scores from baseline to 3rd month within both cohorts (p = .01*). There was also a statistically significant difference in addiction scores between the groups at 2nd (p = .040*) and 3rd month (p = .015*), which is in line with a study conducted by Kumar et al. (2024).
The proportion of self-reported continuous abstinence was higher in the LG than in CG, although lacking statistical significance (p = .238). Over the three-month follow-up period, relapse was noted among participants in both groups, though at a lower rate in the liquorice group. In self-help tobacco cessation interventions, such as behaviour counselling, self-reported continuous abstinence typically ranges between 10% and 25% (Lancaster et al., 2017). The inclusion of a tobacco substitute, such as sugarless chewing gum and liquorice, resulted in an increase in self-reported continuous abstinence rates ranging from 35% to 51%. However, it is important to acknowledge that reliance on self-reported smoking cessation may introduce a bias towards overestimation due to social desirability tendencies. Consequently, the utilization of objective measures is imperative to verify smoking abstinence accurately.
Scientific evidence shows that cotinine, the metabolite of nicotine, persists longer in the body with a half-life in plasma of approximately 16 hours and a half-life in urine of 15–40 hours (Thrul et al., 2018). However, cotinine tests through blood sample collection are invasive, and urine collection is uncomfortable; both necessitate transportation and storage until analysis. Thus, a simple, non-invasive, and scientifically valid exhaled CO measurement with a CO breath analyzer was preferred in the current study. Cunnington and Hormbrey (2002), Deveci et al. (2004), and Shie et al. (2017) found a significant positive correlation between CO levels and daily cigarette consumption. Hence, the usage of a breath analyser for the assessment of exhaled CO is justified.
Nevertheless, the possibility of detection bias remains inherent when employing a CO breath analyzer due to the relatively short half-life of CO in breath, spanning 2 to 6 hours (Nikkholgh et al., 2021). This temporal constraint limits the capability to definitively ascertain the cessation status of participants who abstained from smoking within the 2 to 6 hours preceding the assessment. At the third-month follow-up, the mean CO levels in the LG and the CG were 4.90 ± 2.995 ppm and 6.91 ± 4.512 ppm, respectively. Notably, a statistically significant difference in exhaled CO levels between the LG and the CG was observed at both the second month (p = .046*), and the third month (p = .013*), with the LG exhibiting comparatively lower CO levels. Additionally, a statistically significant reduction in exhaled CO levels from baseline to the third month was evident within both groups (p = .01*). Carbon monoxide (CO) levels showed the greatest reduction at the end of month 1, followed by a slight increase at months 2 and 3. This pattern is most plausibly explained by the study design: the active intervention (liquorice root or chewing gum) was provided only during the first month. After the intervention period ended, participants no longer received the oral-substitution aid, and some likely resumed smoking during follow-up, producing a modest rebound in CO.
In the current trial, even though both sugarless chewing gum and liquorice exhibited notable clinical efficacy in aiding tobacco cessation, liquorice demonstrated superior efficacy over sugarless chewing gum as a substitute for a smoking form of tobacco. Specifically, liquorice exhibited notable efficacy in decreasing tobacco dependence, thereby decreasing the CO levels.
The strength of this study lies in its unique approach, being the first to incorporate liquorice root and sugarless chewing gum as adjuvants in tobacco cessation strategies, specifically in the Indian context. Additionally, the study used natural, readily available liquorice root rather than extracts, powders, or liquids, which require laboratory preparation involving technical resources. This study demonstrates that the interventions can be implemented in real-life situations by the lay public. Randomization was done using a computer-generated random sequence, thereby minimizing allocation bias. Participants were regularly monitored to ensure adherence to the recommended use of the interventions. In addition to in-person follow-up visits, frequent reminder phone calls were made during the study period to reinforce compliance and verify that participants were using liquorice root (3–5 times/day as per craving) and chewing gum (2–3 times/day as per craving) as instructed.
The study has a few limitations. Participants were mainly recruited from a tertiary care hospital’s tobacco cessation centre, as well as through brochures, cessation camps, and outpatient clinics. This recruitment strategy may limit the generalizability of the findings and could have introduced variability in baseline motivation to quit smoking, which was not directly measured. Since motivation strongly influences cessation outcomes, the absence of such an assessment is a noteworthy methodological limitation. Another limitation is the relatively short follow-up period of three months. As relapse rates tend to rise after six months, the long-term effectiveness of the intervention cannot be fully determined.
In addition, although liquorice roots were administered in standardized 1-gram doses, the active ingredient composition of natural products may vary considerably. As the liquorice samples were not chemically analyzed for content, variability in their pharmacological activity cannot be excluded. Finally, the control group received tobacco cessation counselling, which in itself can positively influence smoking cessation outcomes. Including this level of intervention in the control group may have introduced bias, making intergroup comparisons less precise and potentially underestimating the true effect of the liquorice intervention.
Conclusion
In the current trial, even though both sugarless chewing gum and liquorice exhibited notable clinical efficacy in aiding tobacco cessation, liquorice demonstrated superior efficacy over sugarless chewing gum as a substitute for a smoking form of tobacco. Specifically, liquorice exhibited notable efficacy in decreasing tobacco dependence, thereby decreasing the CO levels.
Therefore, when individuals attempt to quit their tobacco habit, it is suggested that pre-cut liquorice could be chewed for 10 to 20 minutes as an adjuvant to counselling. Liquorice can serve as effective substitute for smoking forms of tobacco, aiding in the cessation efforts.
Recommendations
Further long-term follow-up studies should be done to evaluate the effectiveness of liquorice root as an adjuvant to tobacco cessation counselling.
Since liquorice root is found to be effective in smokers, it could also be used as an intervention for the cessation of tobacco among smokeless tobacco users.
Further research may be warranted to explore the mechanisms by which liquorice root exerts its beneficial effects and to provide insights into ways to enhance smoking cessation interventions.
Ethical approval
This study was approved by the Institutional Ethical Review Board (Date: APRIL 26, 2022, Decision/Protocol No: IRB Reference number: 1/IRB/2022). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Carmines, E. L., Lemus, R., & Gaworski, C. L. (2005). Toxicologic evaluation of licorice extract as a cigarette ingredient. Food and Chemical Toxicology, 43(7), 1303-1322. https://doi.org/10.1016/j.fct.2005.03.004
- Cohen, L. M., Collins, F. L., & Britt, D. M. (1997). The effect of chewing gum on tobacco withdrawal. Addictive Behaviors, 22(6), 769-773. https://doi.org/10.1016/S0306-4603(97)00064-0
- Cunnington, A. J., & Hormbrey, P. (2002). Breath analysis to detect recent exposure to carbon monoxide. Postgraduate Medical Journal, 78(918), 233-237. https://doi.org/10.1136/pmj.78.918.233
- Damle, J. M. (2014). Glycyrrhiza glabra (Liquorice) - A potent medicinal herb. International Journal of Herbal Medicine, 2(4), 132-136.
- Deveci, S. E., Deveci, F., Açik, Y., & Ozan, A. T. (2004). The measurement of exhaled carbon monoxide in healthy smokers and non-smokers. Respiratory Medicine, 98(6), 551-556. https://doi.org/10.1016/j.rmed.2003.11.018
- Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerström, K. O. (1991). The fagerström test for nicotine dependence: A revision of the fagerström tolerance questionnaire. British Journal of Addiction, 86(9), 1119-1127. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x
- Kumar, R., Goel, M. K., & Talukdar, T. (2024). Effect of cognitive behavioral therapy on tobacco usage and dependency among adult male tobacco users in Palam area of Delhi. Indian Journal of Community Health, 36(1), 26-32. https://doi.org/10.47203/IJCH.2024.v36i01.006
- Lancaster, T., & Stead, L. F. (2017). Individual behavioural counselling for smoking cessation. Cochrane Database of Systematic Reviews, 3(3), CD001292. https://doi.org/10.1002/14651858.CD001292.pub3
- Ministry of Health and Family Welfare. (2017). Global Adult Tobacco Survey - India - 2016-17 (GATS 2). https://ntcp.mohfw.gov.in/assets/document/surveys-reports-publications/Global-Adult-Tobacco-Survey-Second-Round-India-2016-2017.pdf
- Ministry of Health and Family Welfare. (2018). Establishment of tobacco cessation centers in dental institutes: Operational guidelines. https://dciindia.gov.in/Rule_Regulation/FinaloperationalguidelinesTCCindentalcolleges.pdf
- Mitra, R., Rai, A., Kumar, A., & Mitra, J. K. (2023). Role of herbal medication in tobacco cessation treatment: A systematic review and meta-analysis. Addiction & Health, 15(1), 63-70. https://doi.org/10.34172/ahj.2023.1290
- Naresh, V., Babu, R. R., Prasad, S., & Singh, N. (2016). Pharmacological and non-pharmacological interventions for smoking cessation. International Journal of Preventive and Clinical Dental Research, 3(2), 116-119.
- Nikkholgh, A., Soleimani, M., Torkaman-Boutorabi, A., & Valizadeh, B. (2021). Evaluation of smoking status: Comparison of self-reports with exhaled carbon monoxide analysis in university students in the Islamic Republic of Iran. Eastern Mediterranean Health Journal, 27(4), 321-326. https://doi.org/10.26719/emhj.21.009
- Pastorino, G., Cornara, L., Soares, S., Rodrigues, F., & Oliveira, M. B. P. P. (2018). Liquorice (Glycyrrhiza glabra): A phytochemical and pharmacological review. Phytotherapy Research, 32(12), 2323-2339. https://doi.org/10.1002/ptr.6177
- Shie, H. G., Pan, S. W., Yu, W. K., Chen, W. C., Ho, L. I., & Ko, H. K. (2017). Levels of exhaled carbon monoxide measured during an intervention program predict 1-year smoking cessation: A retrospective observational cohort study. NPJ Primary Care Respiratory Medicine, 27(1), 59. https://doi.org/10.1038/s41533-017-0060-8
- Thrul, J., Meacham, M. C., & Ramo, D. E. (2018). A novel and remote biochemical verification method of smoking abstinence: Predictors of participant compliance. Tobacco Prevention & Cessation, 4, 20. https://doi.org/10.18332/tpc/90649
- U.S. Public Health Service. (2008). Treating tobacco use and dependence: 2008 update. Clinical Practice Guideline. https://www.ncbi.nlm.nih.gov/books/NBK63952/
- World Health Organization. (2024). Tobacco. https://www.who.int/news-room/fact-sheets/detail/tobacco
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.