Abstract
Van, Türkiye’s eastern border province, is a major transit corridor for irregular migrants and lies on the Balkan route for drug trafficking. This study describes the clinical and radiological features of body packer cases presenting to an emergency department in this critical border region. This retrospective case series included all 13 confirmed body packer patients who presented to the University of Health Sciences, Van Training and Research Hospital Emergency Department between January 2021 and November 2025. Data on demographics, clinical presentation, imaging findings, and management were extracted from medical records. Eleven patients (84.6%) were refugees or irregular migrants; all 13 were brought by law enforcement, with no voluntary self-presentations. The median age was 33 years, and 12 were male. The concealed substances were predominantly methamphetamines (69.2%), followed by opioids (15.4%) and cocaine (15.4%). Seven patients (53.8%) were asymptomatic. CT imaging, used in all cases, showed a 100% detection rate. A key finding was the observation of two patients with rectal packet clustering and marked bladder distension, both reporting deliberate avoidance of defecation and urination—a behavioral cue for high-risk screening. The single female patient had multiluminal concealment (rectal and vaginal). No toxicity or mortality occurred; median hospital stay was 3 days. Body packing among migrants in Van is an under-recognized phenomenon at the intersection of migration, trafficking, and substance use vulnerability. The small number of detected cases, all law-enforcement-driven, suggests a significant underestimation of the true burden. The predominance of methamphetamines suggests a significant stimulant trafficking trend. Border-region emergency departments must implement risk-based screening strategies, integrate addiction services, and adopt trauma-informed care frameworks to address the complex needs of this vulnerable population.
Keywords: methamphetamine, body packing, drug trafficking, migration, refugees, emergency management
Main Points
- Body packing among refugees and irregular migrants in Van represents an under-recognized phenomenon at the intersection of migration, trafficking, and substance use vulnerability, with all 13 cases brought by law enforcement and no voluntary presentations.
- Methamphetamines accounted for 69.2% of concealed substances, suggesting a significant shift from the traditional opioid-dominated pattern of the Balkan Route and highlighting evolving regional drug markets.
- Behavioral cues such as deliberate avoidance of defecation and urination leading to bladder distension may serve as practical clinical red flags for risk-based screening in resource-limited border-region settings.
- The absence of major complications and the small number of detected cases over five years suggest that body packing in this region is highly professionalized and that detected cases represent only the “clinical tip of the iceberg.”
- Border-region emergency departments require standardized clinical protocols, trauma-informed care approaches, and integration of addiction services to address the complex medical, psychological, and social needs of this vulnerable population.
Introduction
Body packing, the internal concealment of illicit drugs, places individuals at extreme risk and presents a complex clinical and medico-legal challenge for emergency physicians worldwide (Booker et al., 2009; Cappelletti et al., 2016; Traub et al., 2003). These individuals, often referred to as mules, carry numerous tightly wrapped packets of cocaine, heroin, or other drugs, facing the constant threat of life-threatening toxicity from packet rupture or severe mechanical complications like bowel obstruction (Booker et al., 2009; Traub et al., 2003). While modern packaging has reduced catastrophic ruptures, it has also enabled individuals to travel long distances, often in silence and fear, while remaining asymptomatic (Booker et al., 2009; Maier et al., 2017).
Türkiye stands at a global crossroads of migration. In 2024, the country hosted over 2.9 million Syrians under temporary protection and approximately 194,000 asylum seekers from Afghanistan, Iraq, Iran, and other nations (AIDA, 2025; IOM, 2024). Between 2020 and 2024, Turkish authorities apprehended over 1.3 million irregular migrants, highlighting the sheer scale of human movement across the region (Presidency of Migration Management, 2024).
Van province, situated along the 560-km Türkiye-Iran border, is a primary gateway for irregular migrants from Afghanistan, Pakistan, and Iran on their arduous journey towards Europe (AIDA, 2025). This same geography is a key segment of the Balkan Route, a long-established corridor for Afghan opiates trafficked to European markets (UNODC, 2024, 2025). This convergence places refugees and irregular migrants at a dangerous crossroads, making them exceptionally vulnerable to exploitation by trafficking networks. Previous research has documented the profound links between migration, vulnerability, and substance use disorders in the Turkish context.
While the existing literature on body packing provides valuable diagnostic and management algorithms, it is largely derived from high-income settings (Cappelletti et al., 2016; Fremery et al., 2024; Maier et al., 2017; Traub et al., 2003). The voices and clinical realities of those intercepted in border regions like Van remain underrepresented. This study aims to shed light on the human faces behind the statistics by describing the demographic, clinical, and radiological characteristics of body packer cases presenting to a frontline emergency department.
Our research specifically aimed to address the following question: How does the clinical profile of body packers at a primary border transit hub compare to those reported in destination countries, and what specific medical and behavioral markers can facilitate their early identification? We hypothesized that the profile of body packers in this border region would deviate from traditional patterns, exhibiting a higher prevalence of refugees and a shift towards non-opioid substances, thereby reflecting evolving regional trafficking dynamics.
Methods
Study Design and Setting
This retrospective case series was conducted at the Emergency Department of University of Health Sciences, Van Training and Research Hospital, a tertiary care center in Van, eastern Türkiye. The hospital serves the local population and is the primary receiving facility for apprehended refugees and irregular migrants from the nearby Türkiye-Iran border.
Study Period and Case Identification
The study period extended from January 1, 2021, to November 30, 2025. We identified all patients with confirmed body packing through a systematic review of emergency department logs, imaging reports, and medico-legal consultation records. Search terms included “body packer,” “drug courier,” “internal concealment,” and “packet ingestion.”
Inclusion and Exclusion Criteria
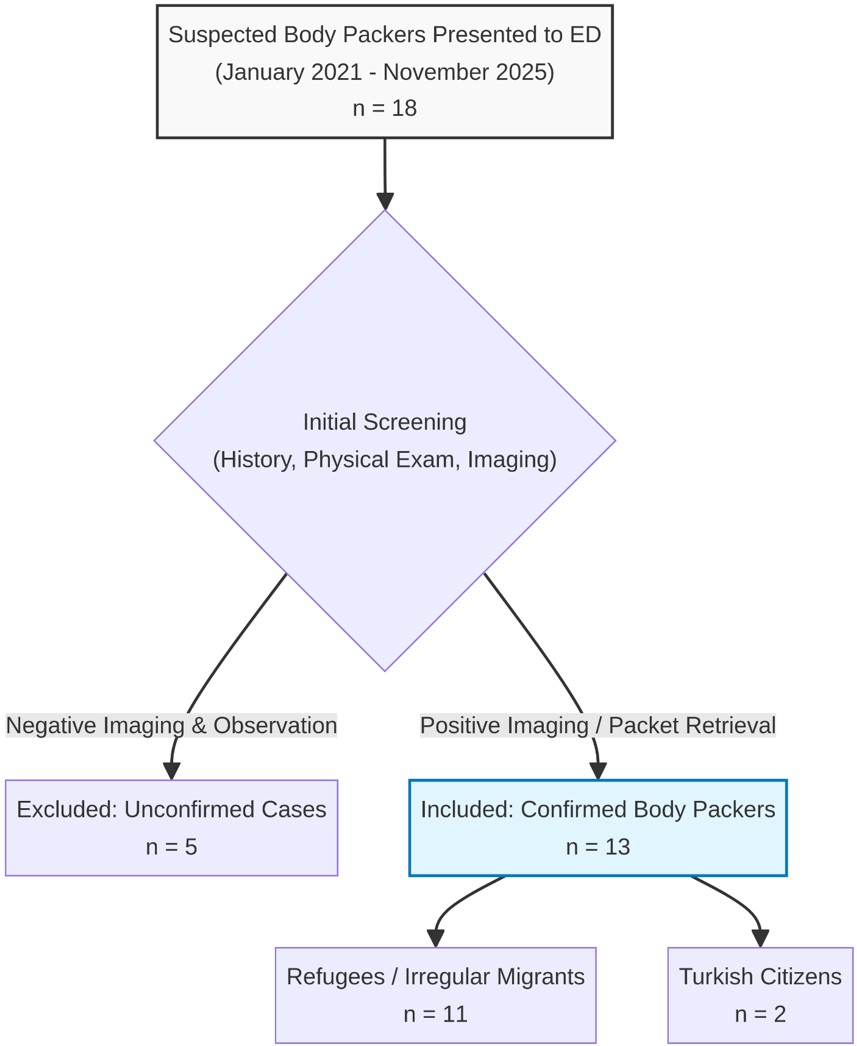
We included all patients aged 18 years or older who visited the Emergency Department during the study period with confirmed cases of body packing. Confirmation was defined by the visualization of foreign bodies resembling drug packets on imaging (plain radiography or CT) or the retrieval of packets, either spontaneously or through intervention. We excluded patients with suspected but unconfirmed body packing (i.e., negative imaging and observation period) and “body stuffers” (individuals who quickly swallow drugs to avoid arrest, typically with loosely wrapped packets). Figure 1 illustrates the study flow and case identification process.
Data Collection
We extracted demographic data (age, sex, nationality, refugee or irregular migrant status), clinical presentation (symptoms, vital signs, route of presentation), laboratory parameters, imaging data (modality, presence and distribution of packets, additional findings), management details, and outcomes. Substance identification was based on forensic laboratory reports provided by law enforcement. We specifically noted rectal packet clustering and bladder distension when reported by radiologists or visible on stored images. Patient reports regarding toileting behavior were extracted from clinical notes when available.
Statistical Analysis
Data were analyzed using descriptive statistics. Continuous variables are presented as medians with ranges (minimum-maximum) due to the non-normal distribution anticipated in small sample sizes. Categorical variables are shown as frequencies (n) and percentages (%). No inferential statistical tests were conducted because of the limited sample size (n=13). All analyses were performed using Microsoft Excel.
Ethical Approval
The study protocol was approved by the University of Health Sciences, Van Training and Research Hospital Ethics Committee (Approval No: GOKAEK/2025-09-03, at date 07.11.2025). All data were anonymized prior to analysis.
Results
Demographic Characteristics
We identified thirteen patients with confirmed body packing. Eleven (84.6%) were refugees or irregular migrants, and two (15.4%) were Turkish citizens. The median age was 33 years (range 22–47 years). Twelve patients (92.3%) were male. The single female patient was a refugee with multiluminal drug concealment involving both the rectum and the vaginal canal.
Concealed Substances
The concealed substances were predominantly methamphetamine, found in 9 cases (69.2%). This category includes 8 cases of methamphetamine and 1 case of methamphetamine combined with THC (tetrahydrocannabinol). Opioids were found in 2 cases (15.4%, including one case combined with THC), and cocaine was found in 2 cases (15.4%). Table 1 summarizes the demographic and clinical characteristics of the cohort.
| CT: Computed tomography. Continuous variables are presented as median (range); categorical variables as n (%). No inferential statistics were performed due to small sample size | |||
| Table 1. Demographic and clinical characteristics of body packer cases (N=13) | |||
| Characteristic |
|
|
|
| Age (years), median (range) |
|
|
|
| Male, n (%) |
|
|
|
| Nationality: Iranian, n (%) |
|
|
|
| Asymptomatic presentation, n (%) |
|
|
|
| CT performed, n (%) |
|
|
|
| Rectal clustering observed, n (%) |
|
|
|
| Bladder distension observed, n (%) |
|
|
|
| Concealed substances | |||
| Methamphetamine-related, n (%) |
|
|
|
| Opioid-related, n (%) |
|
|
|
| Cocaine, n (%) |
|
|
|
| Number of packages, median (range) |
|
|
|
| Multiluminal concealment, n (%) |
|
|
|
| Length of stay (days), median (range) |
|
|
|
| Brought by law enforcement, n (%) |
|
|
|
| Complications or mortality, n (%) |
|
|
|
Clinical Presentation and Vital Signs
Seven patients (53.8%) were asymptomatic upon arrival. Crucially, all 13 individuals were brought to the Emergency Department by law enforcement, a stark finding that indicates a complete absence of self-presentation in this cohort. Among symptomatic patients, abdominal pain (8/13) and nausea/vomiting (4/13) were most common. Vital signs at triage were stable in all patients, with no signs of acute toxicity.
Laboratory Findings
Laboratory parameters were largely unremarkable. Urinary drug screening was performed inconsistently (in 5/13 cases). This inconsistency was due to systemic limitations, the attending physician’s discretion based on clinical suspicion, and varying requests from law enforcement at the time of presentation. However, in cases where it was conducted, it revealed positive results for the concealed substance, suggesting recent exposure or personal use.
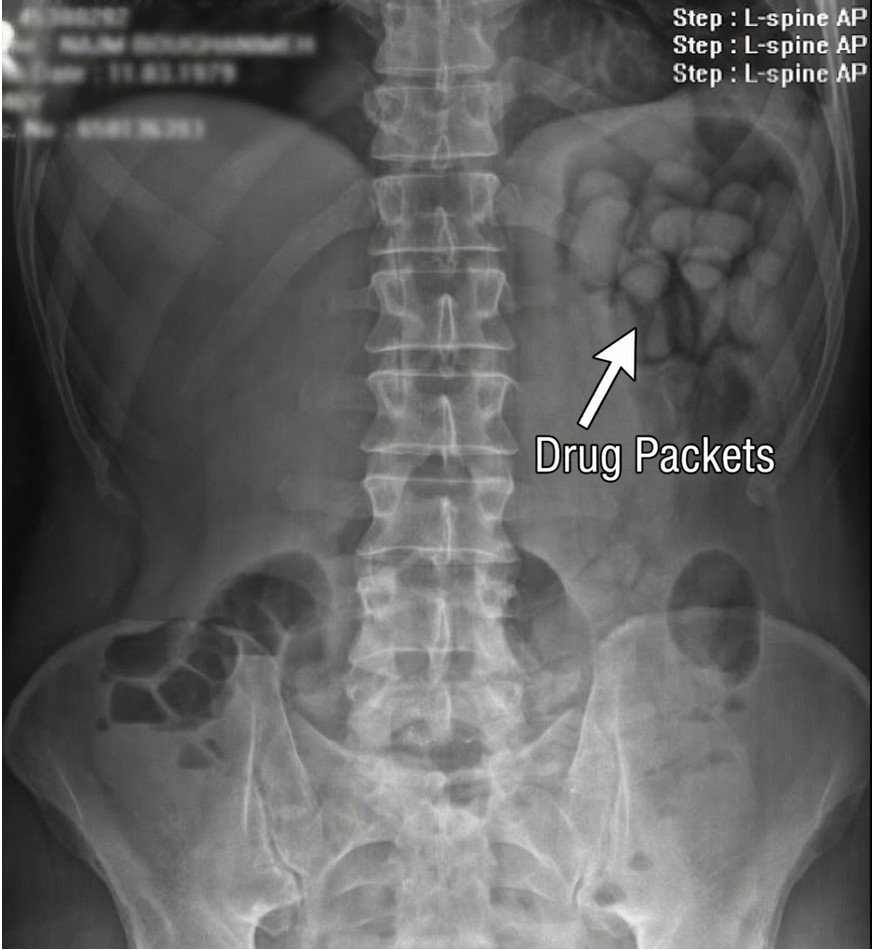
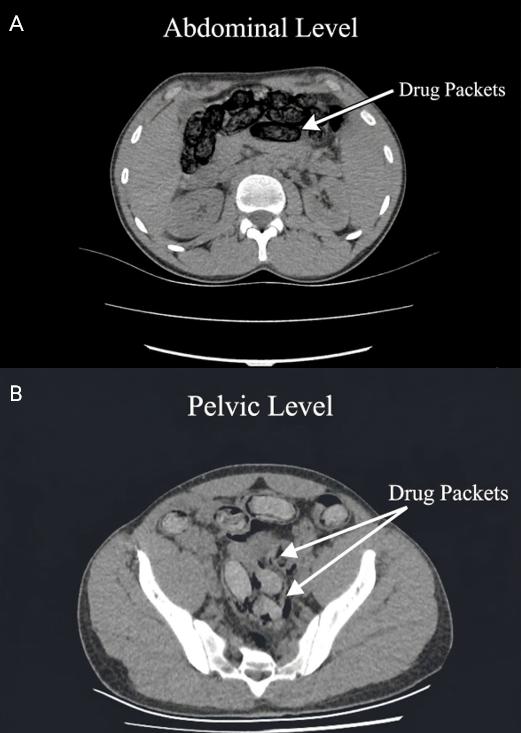
Imaging Findings
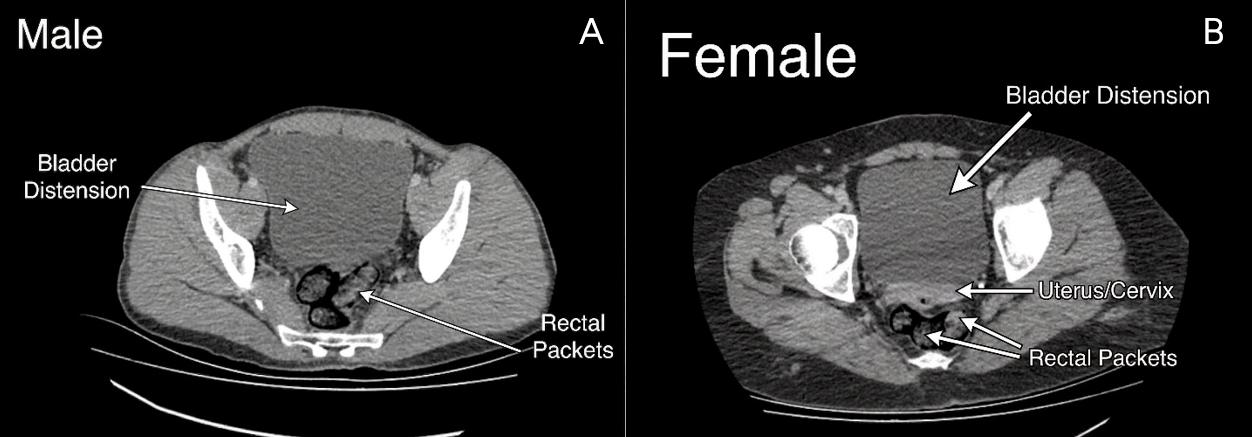
All 13 patients underwent imaging. Plain radiographs demonstrated multiple radiopaque foreign bodies distributed throughout the gastrointestinal tract (Figure 2). CT scans, performed in all cases, provided definitive confirmation with a 100% detection rate for intraluminal packets (Figure 3) (Pinto et al., 2014). No evidence of bowel obstruction or perforation was identified. Two patients exhibited striking pelvic CT findings: multiple oval packets densely clustered in the rectum with markedly distended urinary bladders (Figure 4). Both patients reported deliberately avoiding defecation and urination to prevent packet loss.
Management and Outcomes
Ten patients (76.9%) received whole bowel irrigation (Thanacoody et al., 2015). Four underwent endoscopic intervention, and one required surgery. The median length of hospital stay was 3 days. No patient developed clinical toxicity or died during hospitalization.
Discussion
Our study offers a rare clinical window into the phenomenon of body packing as it unfolds at the dangerous intersection of migration, trafficking, and human vulnerability. The predominance of refugees and irregular migrants in our cohort is a somber reflection of the local migration landscape, where individuals fleeing conflict and poverty are exposed to extreme forms of exploitation.
Van’s strategic position on the Balkan Route, a traditional corridor for Afghan opiates, is well established (AIDA, 2025; UNODC, 2024). While our findings confirm the continued presence of opioids (15.4%), the most striking result is the predominance of methamphetamine (69.2%). This aligns with recent intelligence indicating a significant shift towards stimulant trafficking along the Balkan Route. Multiple reports from the UNODC have highlighted a surge in methamphetamine trafficking along this route in recent years (UNODC, 2025). This finding underscores the evolving nature of stimulant trafficking along the Balkan Route and warrants closer surveillance.
Our clinical findings are consistent with international literature in several respects. The 100% detection rate of CT imaging confirms its role as the diagnostic gold standard (Cappelletti et al., 2016; Fremery et al., 2024; Maier et al., 2017; Traub et al., 2003). Similarly, the favorable clinical outcomes, with no mortality, mirror trends in recent series where improved packaging has reduced catastrophic complications (Cappelletti et al., 2016; Fremery et al., 2024; Maier et al., 2017).
Distinctive Findings and Clinical Implications
The fact that we identified only 13 cases over five years, despite Van being a region with multi-ton annual drug seizures, strongly suggests that these individuals represent the clinical tip of the iceberg. Body packing is a high-risk, high-reward method of trafficking, with a low probability of detection. That all patients were brought in by law enforcement, with no one seeking help voluntarily, paints a stark picture: asymptomatic individuals only enter the healthcare system when intercepted. This reality points to a critical public health gap, leaving the true incidence and human cost of body packing in this region largely invisible. Furthermore, the absence of major complications in our cohort, while clinically fortunate, may suggest a degree of professionalism among traffickers and couriers, implying repeated, successful journeys with well-manufactured packets. However, this interpretation should be approached with caution given our small sample size; it is also possible that we simply did not encounter the complications that undoubtedly occur in this high-risk activity.
The experience of two patients provides a chilling insight into the behaviors driven by coercion and fear. Both individuals intentionally refrained from defecation and urination to avoid packet loss, as instructed by trafficking networks. This manifested radiologically as dense rectal packet accumulation and extreme bladder distension. Frontline clinicians can use signs like persistent toilet refusal, clear discomfort, or defecation anxiety as useful indicators in critical cases.
User vs. Courier: A Critical Distinction
Effectively managing body packers involves a crucial distinction between those who are merely couriers, often under duress, and those who also use substances. Our study’s findings, which include positive urinary drug screens among tested patients, indicate that some couriers are indeed consumers, thereby blurring the line between “packer” and “user.” This differentiation carries significant implications for harm reduction strategies. While a pure courier may need protection and legal advocacy, a courier-user requires immediate attention to withdrawal symptoms and connection to addiction treatment services. The inconsistency in urinary screening identified in our study, attributed to systemic constraints and differences in clinical decision-making, indicates an unrealized opportunity to recognize this patient group. We contend that urinary drug screening should be a standard protocol, not only for legal verification but also to inform clinical management and addiction support.
Limitations and Implications for Clinical Practice
Our study has several limitations inherent to its retrospective, single-center design. The small sample size (n=13), while representing the entirety of confirmed cases at our institution over a five-year period, limits the generalizability of our findings. Our reliance on routine medical records and law-enforcement referrals also introduces the potential for selection and reporting biases. Crucially, due to the retrospective nature of the data, we lacked detailed information on the migrants’ journeys, such as time in transit, specific routes, or the presence of debt bondage or coercion. Future prospective studies should aim to capture these vital sociological details to better understand the drivers of this phenomenon.
Standardization of Clinical Approach
The variation in clinical assessment we observed is not merely a limitation, but a key finding in itself. The inconsistent application of urinary drug screening and CT imaging, alongside incomplete anamnesis, highlights an urgent need for standardized clinical protocols. We propose that such protocols should include routine urinary drug screening for all suspected body packers, systematic CT imaging for high-risk cases, and a detailed, compassionate anamnesis. Adopting such standards would not only improve case detection but also yield more complete epidemiological data to inform public health responses. Crucially, the integration of addiction medicine and mental health services into the care pathway is vital to address the underlying vulnerabilities and trauma experienced by these individuals.
Conclusion
Body packing in the context of migration is not merely a crime; it is a public health crisis born from the convergence of intense migratory flows, established drug-trafficking routes, and profound human vulnerability. Our study provides rare clinical evidence from a key transit hub, challenging the traditional opioid-centric view of the Balkan Route by highlighting a significant prevalence of methamphetamine. While the small number of cases limits broad generalizations, the complete absence of voluntary presentations underscores the hidden nature of this population.
Clinicians on the front lines need more than just technology; they need risk-based screening strategies that integrate a person’s migration context, clinical findings, and behavioral cues. This approach allows for the identification of high-risk individuals while preserving dignity and human rights. Border-region emergency departments must develop structured diagnostic pathways and embed them within trauma-informed, gender-sensitive care frameworks. Ultimately, meaningful progress requires collaboration with public health and migration services to address the broader harms at the perilous interface of migration, trafficking, and addiction.
Ethical approval
This study was approved by the Van Training and Research Hospital Ethics Committee (Date: November, 7, 2025, Decision/Protocol No: GOAEK/2025-09-03). Ethics committee approval and informed consent were not required for this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- AIDA. (2025). AIDA Country Report on Türkiye – Update on 2024. https://ecre.org/aida-country-report-on-turkiye-update-on-2024
- Booker, R. J., Smith, J. E., & Rodger, M. P. (2009). Packers, pushers and stuffers—managing patients with concealed drugs in UK emergency departments: A clinical and medicolegal review. Emergency Medicine Journal, 26(5), 316-320. https://doi.org/10.1136/emj.2008.057695
- Cappelletti, S., Piacentino, D., Sani, G., Bottoni, E., Fiore, P. A., Aromatario, M., & Ciallella, C. (2016). Systematic review of the toxicological and radiological features of body packing. International Journal of Legal Medicine, 130(3), 693-709. https://doi.org/10.1007/s00414-015-1310-3
- Fremery, A., Pujo, J., Aboikoni, A., Hamiche, K., & Bonifay, T. (2024). Body-packing, a public health issue requiring more researches. European Journal of Emergency Medicine, 31(2), 158-159. https://doi.org/10.1097/mej.0000000000001095
- IOM. (2024). Türkiye - Migrant Presence Monitoring, Situation Report, June 2024. Displacement Tracking Matrix (DTM). https://dtm.iom.int/reports/turkiye-migrant-presence-monitoring-situation-report-june-2024
- Maier, L., Trueb, L., Schmidt, S., Carron, P.-N., Hugli, O., Heymann, E., & Yersin, B. (2017). Emergency department management of body packers and body stuffers. Swiss Medical Weekly, 147(3738), w14499 https://doi.org/10.4414/smw.2017.14499
- Pinto, A., Reginelli, A., Pinto, F., Sica, G., Scaglione, M., Berger, F. H., Romano, L., & Brunese, L. (2014). Radiological and practical aspects of body packing. British Journal of Radiology, 87(1036), 20130500. https://doi.org/10.1259/bjr.20130500
- Presidency of Migration Management. (2024). Irregular migration statistics. Republic of Türkiye Ministry of Interior. https://goc.gov.tr/duzensiz-goc-istatistikleri
- Thanacoody, R., Caravati, E. M., Troutman, B., Höjer, J., Benson, B., Hoppu, K., Erdman, A., Bedry, R., & Mégarbane, B. (2015). Position paper update: Whole bowel irrigation for gastrointestinal decontamination of overdose patients. Clinical Toxicology, 53(1), 5-12. https://doi.org/10.3109/15563650.2014.989326
- Traub, S. J., Hoffman, R. S., & Nelson, L. S. (2003). Body packing-the internal concealment of illicit drugs. New England Journal of Medicine, 349(26), 2519-2526. https://doi.org/10.1056/NEJMra022719
- UNODC. (2024). Findings of the expert working group on opiates and methamphetamine trafficking on the southern route. United Nations Office on Drugs and Crime.
- UNODC. (2025). Opiates and methamphetamine trafficking on the balkan route: Drug flows, illicit incomes and illicit financial flows. United Nations Office on Drugs and Crime.
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.