Abstract
Refugees face a unique constellation of pre-, peri-, and post-migration stressors that can increase vulnerability to hazardous substance use while simultaneously limiting access to appropriate care. To address this gap, the PREPARE consortium was established as the first coordinated German research network on substance use among refugees, combining empirical assessment, diagnostic innovation, and intervention development. This article provides an overview of the network and synthesizes cross-project learnings with a particular focus on Subproject 4 (STARC-SUD), an emotion-regulation–based group intervention adapted for refugees with hazardous alcohol or drug use.
Across multiple sites, PREPARE identified substantial barriers to recruitment and engagement, including stigma, legal insecurity, language difficulties, and the structural conditions of communal accommodation. The adaptation and translation of screening instruments improved diagnostic accuracy, while iterative modifications of STARC-SUD enhanced cultural fit and feasibility. Early implementation experiences highlight the importance of trust-building, flexible delivery formats, and close cooperation with community actors. The Sucht-und-Flucht.de platform (https://www.sucht-und-flucht.de/en/) emerged as a central dissemination tool, providing multilingual materials, diagnostic instruments, and project information to practitioners and supporting long-term knowledge transfer.
The preliminary observations from the ongoing trial underscore the need for integrated, culturally sensitive, and trauma-informed approaches within European addiction-care systems. PREPARE demonstrates the potential of emotion-regulation interventions for refugee populations and points to the importance of sustained, multi-level strategies involving research, practice, and policy to improve access and outcomes for displaced individuals affected by substance use.
Keywords: addictions to alcohol, addictions to drugs, alcohol, germany, mental heath, prevention, refugees
Main Points
- PREPARE is a multi-site German research consortium integrating complementary subprojects across institutions to advance understanding, assessment, and care of substance use among refugees.
- Across subprojects, refugees with hazardous substance use emerged as a highly underserved and hard-to-reach group due to stigma, legal insecurity, language barriers, and unstable living conditions.
- Culturally adapted screening tools and multilingual materials are essential for improving diagnostic accuracy and access to addiction care for refugee populations.
- STARC-SUD provides a culturally sensitive, trauma-informed group intervention linking emotion regulation with substance-use behavior in refugees with hazardous alcohol or drug use.
- The Sucht-und-Flucht.de platform facilitates sustainable knowledge transfer by offering multilingual resources, diagnostic instruments, and practice-oriented materials for professionals.
Introduction
Refugee Migration and Substance Use: The German Context
While refugee migration to Germany had already been rising in the years before, 2015 marked a significant increase, particularly among people from Syria, Afghanistan, and Iraq. This demographic shift has drawn attention to the complex health needs of these populations, including the often-overlooked domain of substance use. Research indicates that forced migrants are exposed to a combination of pre-migration traumatic events, stressful displacement trajectories, and post-migration stressors – such as legal uncertainty, unemployment, social marginalization, and discrimination – which jointly contribute to elevated vulnerability for mental health problems and risk-related behaviors (Chen et al., 2017; Hajak et al., 2021).
Despite these risks, population-level data on substance use patterns among refugees in Germany remain scarce. Studies consistently highlight diagnostic challenges, limited culturally validated screening tools, and significant heterogeneity across refugee subgroups, making it difficult to establish reliable prevalence estimates (Ezard, 2012). Qualitative research suggests that substance use among displaced populations may serve as a maladaptive coping response to trauma and ongoing stressors, yet it also reflects culturally embedded meanings, social norms, and gendered expectations (Lindert et al., 2021).
At the same time, refugees access addiction services at significantly lower rates than the general population, a phenomenon repeatedly described as one of the core structural challenges in German addiction care (Schwarzkopf et al., 2023; von Glahn-Middelmenne, 2023). Structural barriers include complex administrative requirements, language barriers, limited availability of interpretation services, lack of knowledge about the health system, and the separation between psychiatric/trauma services and addiction treatment sectors (Boettcher et al., 2021; Kiselev et al., 2020).
Taken together, the available evidence underscores both the relevance and urgency of developing targeted, culturally sensitive approaches to better understand and address substance use among refugees in Germany. It also highlights the substantial knowledge gaps, particularly regarding prevalence, assessment, and pathways into care—gaps which the PREPARE research network seeks to address.
Unaccompanied Young Refugees
Young refugees entering adulthood face a range of vulnerabilities. The Council of Europe defines “young refugees in transition to adulthood” as those who arrived as children and have since reached adulthood, emphasizing their heightened exposure to exclusion, violence, and unmet rights if adequate support structures are lacking (Council of Europe, 2019).
Research across disciplines, including psychological and ethnographic perspectives, has shown that young refugees—especially when unaccompanied or separated from caregivers—constitute a subgroup frequently described as particularly vulnerable due to their exposure to traumatic events, uncertainty, and precarious living conditions. At the same time, studies also document their resilience and agency, highlighting that vulnerability and capability coexist and shape the experiences of young people on the move (Lems et al., 2020; Müller-Funk et al., 2023; Uzureau et al., 2024).
Research consistently shows high burdens of mental health problems among unaccompanied young refugees. Meta-analytic and systematic evidence indicates an elevated prevalence of post-traumatic stress, depression, and anxiety disorders in this group, driven by both traumatic exposures and daily post-migration stressors (Blackmore et al., 2020; Pfeiffer et al., 2022). Other studies point to profound risks of loneliness and social isolation, which are exacerbated when young people are separated from their families or lack stable social networks in the host country (Garcia & Birman, 2022; Nguyen et al., 2024).
These stressors can overwhelm coping capacities and increase susceptibility to maladaptive coping behaviors, including problematic substance use (Aleer et al., 2023). This is particularly problematic for young people who are still in development (Sweeney et al., 2018). Evidence suggests that although alcohol use among migrant youth is often lower than among their native-born peers, patterns for tobacco and illicit drugs vary across groups and contexts (van Dorp et al., 2021).
Taken together, these findings underline the particular importance of developing culturally sensitive, developmentally informed prevention and intervention strategies for young refugees—especially those who arrived unaccompanied—to address their unique combinations of resilience, risk, and unmet service needs.
Need for Culturally Sensitive and Integrated Approaches
Research demonstrates that mainstream addiction services in Europe often fail to reach refugees and other people with migration backgrounds. Early German literature criticized a deficit-oriented perspective, which tended to attribute low uptake of addiction services to refugees’ “otherness” rather than to systemic factors. In a monograph that helped shape the debate, Penka argues that such a view overlooks how fear of stigma, mistrust of Western health systems, unfamiliarity with available services, and divergent explanatory models of addiction discourage migrants from seeking help (Penka, 2004). Subsequent studies across Europe have documented additional structural and socio-cultural barriers, including inadequate funding for interpretation, cumbersome administrative processes, discriminatory attitudes, and the fact that entitlement to addiction treatment varies by legal status and federal state (Kiselev et al., 2020; Penka et al., 2015). Qualitative studies with Syrian male refugees in Germany echo these findings, noting that negative perceptions of psychiatry, lack of trust in clinicians, and uncertainty about their rights reduce the likelihood of accessing addiction services (Lindert et al., 2021).
These barriers are compounded by the limitations of existing screening tools and interventions. Standardized instruments for substance use assessment are typically developed and validated in Western populations. As a result, they may not capture culturally specific expressions of distress, explanatory models, or idioms of substance use. Penka and colleagues describe how differences in conceptualizing suffering and addiction can lead to misunderstandings in clinical encounters and misclassification of symptoms (Penka et al., 2012). International frameworks for cultural adaptation stress that effective interventions must modify language, content, and delivery to align with the target group’s cultural patterns and values; such adaptation significantly improves acceptability and outcomes (Bernal et al., 2009). Empirical work with refugees further highlights the need for trauma-informed approaches that integrate substance-use and mental-health treatment, rather than importing Western models unchanged (Penka et al., 2015).
Beyond clinical practice, the political and health-system relevance of culturally sensitive approaches is widely acknowledged. A Europe-wide Delphi study found broad consensus that migrants and refugees should have equal access to health insurance, interpretation services, and non-discriminatory care, but revealed disagreement over how health systems should engage with cultural differences (Devillé et al., 2011). Calls for “intercultural opening” have circulated in Germany since the 1990s, advocating organizational change, multilingual outreach, and recruitment of staff with migration backgrounds to ensure equitable access to addiction services (Penka et al., 2015). Yet national data indicate that people with migration backgrounds remain underrepresented in addiction care, and usage statistics often fail to record refugees as a separate category, limiting the visibility of their needs (Kuhn et al., 2018; Leicht & Köhnlein, 2018). These findings underscore the imperative for integrated, culturally adapted prevention and treatment models – an imperative that the PREPARE research network seeks to meet.
Aim of This Article
This article has three interlinked aims, corresponding to the overarching logic of the PREPARE consortium and the current state of implementation across its subprojects: (1) to present the structure of the PREPARE-network, (2) to summarize early cross-project learnings from implementation, coordination, recruitment, and cultural adaptation, and (3) to highlight the subproject STARC-SUD as a key component of PREPARE, focusing on emotion regulation in forced migrants with substance use problems.
The PREPARE Research Network
Background and Funding Context
The German Federal Ministry of Education and Research (BMBF) responded to the large influx of refugees in 2015/2016 by launching the funding call “Forschungsverbünde zur psychischen Gesundheit geflüchteter Menschen” (“Research networks on the mental health of refugees”). This program, initiated in late 2016, emphasized the need for patient-oriented, interdisciplinary consortia to develop culturally sensitive assessment, prevention, and treatment approaches for refugees. The funded networks were intended to produce evidence-based solutions for mental health care and to collaborate across disciplines and regions.
PREPARE – “Prevention and Treatment of Substance Use Disorders in Refugees” – was selected as one of seven consortia. While the BMBF call addressed refugee mental health broadly, PREPARE specifically targets the intersection of forced migration and substance use. It is coordinated by the Center for Interdisciplinary Addiction Research (ZIS) at the University Medical Center Hamburg-Eppendorf (UKE), with partners in Berlin, Cologne, Emden/Leer, and the German Centre for Addiction Issues (DHS). Together with multiple addiction counselling and treatment facilities in Hamburg, Bremen, Berlin, Hanover, Frankfurt, and Munich, PREPARE integrates epidemiological surveys, qualitative studies, and intervention trials.
The consortium pursues four core objectives: (1) to provide systematic evidence on substance-use problems among refugees in Germany; (2) to identify principles of good practice for addiction care and develop culturally adapted assessment instruments; (3) to test innovative interventions for indicated prevention, and (4) to evaluate an integrative, emotion-regulation–based group treatment for refugees with traumatic experiences and substance-use disorders. The findings and materials generated by PREPARE are already disseminated via a national web-based resource center hosted by the German Centre for Addiction Issues.
Network Structure and Partnerships
The PREPARE consortium is a multi-institutional network that brings together research, clinical, and practice partners across Germany. The core academic members are the Center for Interdisciplinary Addiction Research (ZIS) at the University of Hamburg, which houses the overall coordination; the Department of Psychiatry and Psychotherapy at Charité – Universitätsmedizin Berlin; the Faculty of Social Work and Health at the University of Applied Sciences Emden/Leer; the German Institute on Addiction and Prevention Research at the Catholic University of Applied Sciences in Cologne; and the Distributed Artificial Intelligence Laboratory at Technical University Berlin. In addition, the German Centre for Addiction Issues (Deutsche Hauptstelle für Suchtfragen, DHS) acts as a dissemination partner by cooperating with ZIS in developing the nationwide platform for practice integration and knowledge transfer. These academic and dissemination partners work closely with practice organizations and service providers in a range of metropolitan regions – including Berlin, Hamburg, Hanover, Bremen, Cologne, Nuremberg, Stuttgart, Frankfurt, and Munich.
Overview of the Four Subprojects
TP1 – Prevalence, Service Use and Good Practice
The first subproject, based at Charité – Universitätsmedizin Berlin (Prof. Dr. Dr. A. Heinz, Dr. S. Penka) aims to quantify how many refugees in Germany meet criteria for hazardous or dependent substance use, identify groups with heightened risk, and assess whether existing services reach them. Employing the World Health Organization’s Rapid Assessment and Response (RAR) methodology, the team assembled contextual data, established local networks, and conducted 108 semi-structured interviews with staff from refugee facilities, addiction services, and community organizations; findings were validated through focus groups and a consensus-driven Delphi process involving 22 experts. This process yielded a handout outlining 39 “good practice” strategies across nine domains (e.g. organizational structures, multilingual information, outreach, and staff training) to help addiction services better engage refugees. The project addresses the longstanding observation that prevalence estimates of substance use among refugees vary widely and that systematic data on service utilization have been scarce.
TP2 – Assessment and Cultural Adaptation of SUD Instruments
The second subproject, led by the University of Applied Sciences Emden/Leer (Prof. Dr. J. Lindert), responds to the lack of culturally validated screening tools for substance use in refugee populations. Its goals are to conduct a systematic review of existing instruments, identify a measure judged valid by experts and refugees, and then adapt this instrument to the cultural and linguistic context of Syrian refugees. The adaptation process follows established guidelines for cross-cultural translation and psychometric equivalence, using Delphi panels and focus groups to ensure semantic and conceptual alignment. An initial product is a collection of multilingual diagnostic instruments, already publicly accessible on the web-based platform.
TP3 – Smartphone-Based Indicated Prevention
The third subproject, carried out by the German Institute on Addiction and Prevention Research (Prof. Dr. M. Klein) and the Distributed Artificial Intelligence Laboratory at TU Berlin (Prof. Dr. Dr. S. Albayrak), develops BePrepared, a smartphone app designed for young refugees from Syria, Iraq, and Afghanistan who engage in risky alcohol or cannabis use. The app combines four core modules – (1) a consumption diary for self-monitoring, (2) motivational exercises to support change, (3) cognitive-behavioral techniques (e.g. refusal-skills training) and (4) relaxation and affect regulation—plus optional psychoeducation and information about local services. This design is informed by evidence that personalized digital interventions can reduce hazardous drinking and cannabis use as effectively as face-to-face programs.
TP4 – Emotion-Regulation Group Treatment (STARC-SUD)
The fourth subproject, coordinated by the Center for Interdisciplinary Addiction Research (ZIS) in Hamburg (Prof. Dr. I. Schäfer, Prof. Dr. A. Lotzin), adapts the Skills Training in Affect Regulation – a Culture-Sensitive Approach (STARC) for refugees with substance-use problems and trauma-related distress. The original STARC program combines cognitive-behavioral therapy with narrative techniques and culturally resonant metaphors and has shown positive effects on emotion regulation in young Afghan refugees. STARC-SUD extends this model by adding modules on substance-use psychoeducation, motivational enhancement, self-reflection, and relapse prevention, developed in close collaboration with refugees and clinicians. A multi-site randomized controlled trial will compare STARC-SUD to treatment as usual among male refugees with hazardous substance use and trauma exposure, with outcomes including psychological distress, emotion regulation, and substance-use behavior.
Early Cross-Project Learnings from PREPARE
Recruitment Barriers Across Sites
The earliest and most comprehensive assessment of recruitment challenges within the PREPARE network comes from the multi-site rapid assessment conducted by Penka and colleagues (Hertner et al., 2023). Across 108 key-informant interviews and 10 focus groups, the authors showed that refugees with hazardous or dependent substance use constitute an extremely hard-to-reach population. Direct recruitment attempts repeatedly failed because individuals feared negative legal consequences, including repercussions for their asylum procedure, and because substance use carries a dual stigma – both as a refugee and as someone who uses alcohol or drugs. Due to these barriers, the study relied heavily on snowball sampling and gatekeeper-mediated access, and noted that recruitment outside large cities was particularly difficult, as expertise and service structures were far less developed.
These barriers quickly became apparent across all other PREPARE subprojects as well. The assumption – common in early project planning – that young refugees could be reached efficiently through digital means proved overly optimistic. In TP3 (BePrepared), many participants had unstable phone access, limited data plans, or insufficient digital literacy, and promotional campaigns did not translate into spontaneous self-enrollment. Recruitment ultimately required trained cultural brokers who conducted in-person outreach and mobilized peer networks, demonstrating that smartphone affinity alone is insufficient to reach this group.
TP4 (STARC-SUD) also encountered difficulties in recruiting. Pandemic-related restrictions delayed all early activities, but even after restrictions were lifted, it remained extremely difficult to persuade men living in shared accommodation to join a ten-session group therapy program. Many had unstable daily routines, limited privacy, responsibilities towards family members abroad, or were overwhelmed by the bureaucratic burden of asylum procedures. These realities made it difficult to commit to weekly sessions or to reliably attend. Furthermore, the chaotic and often noisy living environment in reception centers – lack of sleep, overcrowded rooms, ongoing conflicts, persistent uncertainty – left little psychological space for proactive help-seeking.
Across the network, it became evident that recruitment challenges had been systematically underestimated. Structural barriers – fragmented services, limited interpretation resources, lack of multilingual staff, mobility restrictions, and legal uncertainties – combined with personal and social barriers such as stigma, mistrust, and fear of institutional contact. PREPARE’s experience underscores that future interventions must invest far more in outreach, cultural brokerage, trust-building, and tailored recruitment strategies that address the living conditions of refugees in collective accommodation. Digital solutions, while promising, cannot substitute for sustained personal engagement, relationship-building, and community-based recruitment infrastructures.
Language, Interpretation, and Communication Challenges
Language and communication barriers emerged as a central challenge across several PREPARE subprojects. A nationwide survey of German addiction services showed that institutions rarely implement resource-intensive strategies such as multilingual information, interpreter use, or employment of staff with migration backgrounds. Instead, many services restrict themselves to low-cost measures that require no additional resources, such as offering general information without translation, because interpreter services and multilingual materials are too costly for most facilities (Stylianopoulos et al., 2023). Respondents consistently identified lack of funding for interpreters and the organizational workload involved in coordinating language mediation as major obstacles to adequate care (Stylianopoulos et al., 2023). These findings are reflected in the PREPARE Delphi study, in which experts again emphasized that interpreter costs and organizational burden significantly limit both access and treatment quality.
The case-control study on addiction-service usage highlighted that refugees face language, monetary, and social barriers, often compounded by limited knowledge of the German health system. As a result, refugees struggle to understand available services and frequently do not access addiction treatment at all (Lopez-Atanes et al., 2025).
Cultural Considerations and Adaptation Needs
Cultural norms, gender expectations, and community-based attitudes toward substance use shaped both participants’ help-seeking behaviors and the feasibility of implementing PREPARE interventions. Qualitative research on Syrian male refugees demonstrates that substance use is embedded in culturally specific understandings of masculinity, strength, and emotional restraint. In this context, emotional vulnerability may be difficult to accept, while anger can be a more socially acceptable expression of distress (Lindert et al., 2021). The same study highlights the role of honor, shame, and social reputation, which strongly influence whether individuals admit substance use or participate in treatment.
These patterns were directly relevant for the adaptation of the STARC-SUD intervention. As described in the adaptation process, the team needed to restructure materials to include culturally resonant metaphors, reduce direct confrontation of emotional topics, and integrate examples reflecting participants’ lived experiences—such as displacement-related stress, family obligations abroad, and culturally normed emotional suppression. Focus groups revealed that men often associated emotional expression with weakness, making psychoeducation about emotion regulation especially important (Lotzin et al., 2021).
Across PREPARE sites, shame and stigma emerged as key cultural barriers. Many participants feared negative judgement within their ethnic or religious communities, particularly in cases of alcohol use (prohibited in Islam), which created pressure to conceal substance-related problems. These dynamics were also identified in the Delphi study, where experts noted that refugees’ fear of social sanctions, moral judgement, and loss of status within family or community reduced both treatment engagement and participation in preventive interventions. Where appropriate, cultural and religious frameworks, including Islamic beliefs, were considered in the adaptation of intervention materials and communication strategies to enhance acceptability and relevance.
This dynamic is further complicated by the widespread anti-immigrant sentiment and anti-Muslim racism in Germany, adding another layer of stigmatization. This affects not only everyday social interactions but also shapes encounters with care providers (Dumke & Neuner, 2023) and needs to be considered when implementing any intervention in this context.
For future interventions, PREPARE’s experience underscores the importance of culturally grounded adaptation – including flexible session structures, sensitive handling of emotion-focused content, and the integration of narratives reflecting gender roles, stigma, and community norms. Without such adaptation, interventions risk missing their target group or failing to address the deeper cultural dynamics that shape substance use and recovery.
The Emotion-Regulation–Based Intervention STARC-SUD
Rationale for Combining SUD and Emotion Regulation
The rationale for viewing emotion regulation as a core mechanism in trauma-related substance use derives from a substantial body of evidence showing that individuals exposed to trauma frequently use alcohol or drugs to down-regulate overwhelming negative affect. Meta-analytic research demonstrates that difficulties in emotion regulation occur across numerous mental disorders and significantly contribute to the onset and maintenance of substance-use disorders (Aldao et al., 2010). This mechanism aligns with the self-medication hypothesis, which proposes that substances are used to dampen sadness, anger, fear, or intrusive trauma-related emotions. Additional reviews confirm that emotion-regulation impairments are strongly associated with both craving and relapse risk (Weiss et al., 2022). Among refugees, this mechanism is intensified by ongoing post-migration stressors—uncertainty in asylum procedures, discrimination, unemployment, and social isolation—which elevate emotional distress and increase reliance on substances as maladaptive coping (Schäfer et al., 2022).
Evidence from prior STARC trials underscores why emotion-regulation treatment forms a strong empirical foundation for STARC-SUD. The original STARC approach, developed by Koch and Liedl, was designed as a culturally sensitive 14-session group intervention teaching emotion recognition, cognitive and behavioral regulation strategies, and coping with specific emotion categories such as anger and fear. A pilot randomized controlled trial with young Afghan refugees demonstrated that STARC significantly improved emotion regulation and reduced psychological distress and PTSD symptoms (Koch et al., 2020). However, the original STARC did not address substance-use behavior directly. The PREPARE consortium therefore expanded the model into STARC-SUD, integrating SUD-specific psychoeducation, motivational components and relapse-prevention elements – while preserving the core transdiagnostic focus on emotional processes of STARC (Lotzin et al., 2021).
The relevance of an emotion-regulation-based intervention for male refugees is particularly well supported by qualitative evidence. A study of Syrian male refugees in Germany found that many participants used alcohol, cannabis, or sedatives to manage intrusive memories, anxiety, anger, and daily stress, and that these patterns were deeply shaped by cultural scripts (Lindert et al., 2021). Emotional suppression was described as a normative expectation, making adaptive regulation strategies unfamiliar or inaccessible. Substance use therefore frequently served as a culturally sanctioned alternative to showing vulnerability. Beyond these cultural dynamics, epidemiological work shows that young men from conflict-affected regions experience disproportionate trauma exposure and elevated risk for both PTSD and SUD. By teaching culturally sensitive strategies for articulating, understanding, and regulating emotions, STARC-SUD targets both the psychological mechanisms that drive trauma-related substance use and the gendered cultural norms that shape help-seeking behavior.
This evidence supports the adaptation of the original STARC intervention for refugees with substance-use disorders by embedding SUD-specific psychoeducation and coping strategies into its established emotion-regulation model. Emotion dysregulation is a central mechanism linking trauma to substance use; STARC has demonstrated feasibility and clinical impact in refugee populations; and qualitative research highlights the specific vulnerability – and specific needs – of male refugees. For these reasons, STARC-SUD represents a theoretically grounded and culturally responsive intervention within the PREPARE research network.
Development and Cultural Adaptation of STARC-SUD
The development of STARC-SUD followed a structured cultural adaptation process grounded in established frameworks for modifying psychological interventions for refugee populations (Heim & Kohrt, 2019). The team conducted five focus groups with Syrian male refugees to explore cultural understandings of substance use, emotional expression, and help-seeking. Themes derived from inductive content analysis informed an expert panel’s adaptation proposals, which were refined through consensus discussions. A preliminary version of the adapted manual was then piloted in two therapy groups, and therapist feedback guided further revisions (Lotzin et al., 2021). These steps resulted in several structural adjustments – notably the reduction from 14 to 10 sessions, the retention and simplification of cultural metaphors (Koch & Liedl, 2019), and the addition of introductory psychoeducation on group-therapy principles to address initial unfamiliarity with Western therapeutic formats.
Further adaptations targeted cultural norms and gender-specific preferences. Focus-group participants identified certain activities in the original STARC manual as culturally incongruent for male groups, prompting the inclusion of alternatives more aligned with participants’ expectations. Because emotional distress was managed in diverse ways, the program now offers both active (e.g., physical movement, singing) and passive (e.g., breathing exercises, grounding) regulation techniques, allowing facilitators to tailor exercises to individual and cultural preferences. The manual also advises therapists to incorporate religious or spiritual elements only upon request, acknowledging the diversity of religious identities among Syrian refugees (Lotzin et al., 2021).
A major innovation of STARC-SUD was the introduction of content specific to substance use. Psychoeducation on addiction as a mental health condition, motivational elements, and relapse-prevention strategies were added to enhance relevance for participants with hazardous use or diagnosed SUD. Sessions now explore risk and protective factors – including trauma, discrimination, family separation, and community support. Throughout the program, SUD-related examples reinforce the core principle that substance use often functions as maladaptive emotion regulation. To make these patterns visible, participants learn to break down situations step by step – identifying what happened before the urge to use, which emotions and thoughts were involved, and how this led to substance use. This step-by-step reconstruction, often referred to as chain analysis, helps them understand where alternative coping strategies can be applied (Lotzin et al., 2021).
These adaptations transformed STARC into a culturally attuned and clinically relevant intervention for refugees with substance-use disorders, maintaining the program’s central focus on emotion regulation while integrating language, metaphors, and therapeutic elements that reflect the lived experiences of the target population.
Structure and Content of the Intervention
STARC-SUD is delivered as a manualized group intervention, typically involving six to eight participants with an interpreter present when needed. Each weekly session lasts around 90 minutes and follows a clearly structured sequence designed to foster predictability and a sense of safety for participants (Lotzin et al., 2021). The intervention is organized around four thematic elements derived from the original STARC program: building emotional awareness, learning and practicing regulation strategies, working with specific emotions, and concluding with consolidation and planning (Koch & Liedl, 2019).
The adapted manual integrates these elements with content specific to substance use, making clear connections between emotional distress and consumption patterns. Participants receive psychoeducation on addiction as a mental health condition and discuss how trauma, discrimination, and separation from family can influence both emotions and substance use (Lotzin et al., 2021). They practice cognitive and body-based regulation techniques, explore culturally familiar coping alternatives, and work with examples illustrating how maladaptive emotion regulation can lead to use. In several sessions, participants break down real-life situations step by step – examining triggers, thoughts, feelings, and behaviors – to better understand the pathways leading to substance use; this stepwise reconstruction is introduced as chain analysis (Lotzin et al., 2021). The manual also includes motivational elements and relapse-prevention strategies informed by evidence from group therapy for SUD.
Therapists delivering STARC-SUD receive dedicated training to ensure consistent implementation. Before leading groups, they complete an intensive training conducted by the program developers, covering the manual, cultural considerations, and the integration of SUD-related content (Schäfer et al., 2022). Ongoing supervision and regular team meetings support fidelity throughout the intervention. Interpreters, who play a central role in facilitating communication, are briefed before sessions and receive written instructions to ensure accurate and culturally appropriate translation of key concepts (Lotzin et al., 2021). They also assist during assessment procedures to maintain consistency and comprehension (Schäfer et al., 2022).
These elements make STARC-SUD a structured, accessible, and culturally responsive intervention that combines emotion-regulation training with components specific to substance use tailored to the needs of refugee men with hazardous or dependent use.
Study Design of the Ongoing RCT
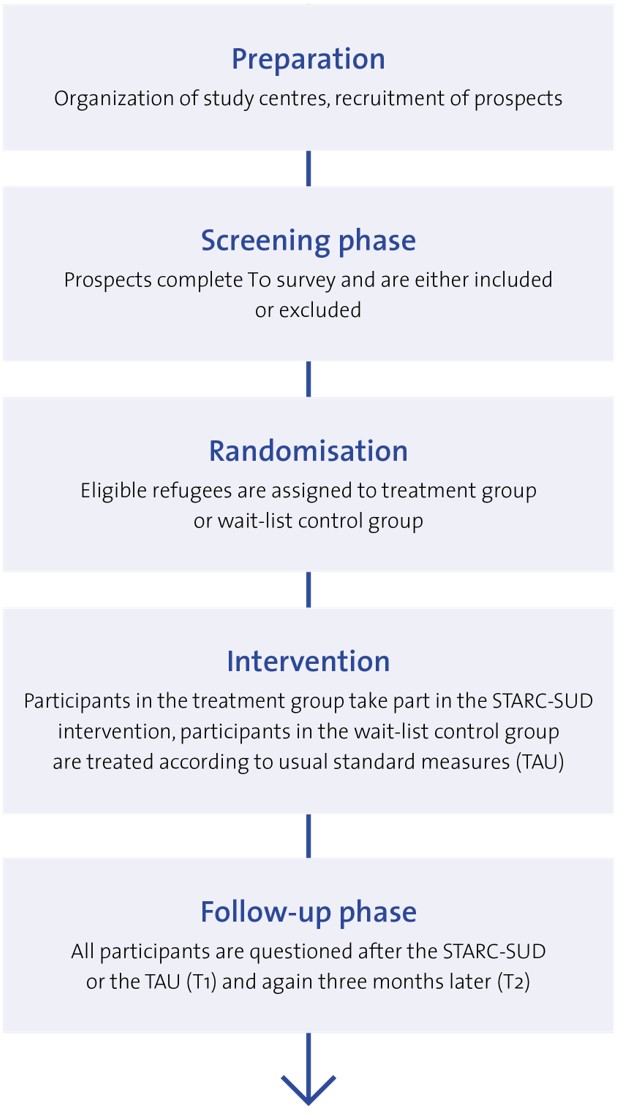
The effectiveness of STARC-SUD is currently being examined in a multicenter, randomized controlled trial conducted across different German metropolitan regions. The trial started in Hamburg, Bremen, Berlin, Hanover, Frankfurt, and Munich (Schäfer et al., 2022). Later, sites in Nuremberg, Stuttgart and Essen joined it. The study aims to recruit 286 male refugees who exhibit psychological distress and hazardous substance use or a substance-use disorder (Schäfer et al., 2022). Participants must be asylum seekers or refugees from countries such as Afghanistan, Syria, or Iraq, and must have experienced war, persecution, or flight-related trauma (Schäfer et al., 2022). A brief screening interview assesses these criteria; men with acute psychosis or acute suicidality are excluded. Eligible individuals are randomly assigned to either the STARC-SUD intervention or a treatment-as-usual control group. Randomization takes place in blocks to ensure balanced allocation across sites.
The trial is designed as a feasibility and effectiveness study. STARC-SUD is delivered in group sessions at addiction-counselling and treatment centers, with therapists supported by interpreters. Participants attend a baseline assessment (t₀), complete the intervention over several weeks, and are re-assessed at the end of treatment and three months later. Each assessment includes measures of general psychological distress, emotion-regulation difficulties, substance use, and post-traumatic stress symptoms (Schäfer et al., 2022). These assessment points and the overall study flow are shown in Figure 1, which illustrates the timeline from preparation to recruitment, randomization, and completion of the intervention.
The trial does not collect biological samples and permits participants to access routine medical and counselling services alongside the study (Schäfer et al., 2022). Materials are provided in simplified Arabic, Farsi, and English, informed consent is carefully explained and documented, and participants can withdraw at any time (Schäfer et al., 2022). Severe symptoms during the study allow for immediate referral or discontinuation. Therapists receive intensive training and ongoing supervision to ensure fidelity, and interpreters support both intervention and assessment with preparatory briefings to ensure accurate and culturally attuned translation (Lotzin et al., 2021).
Early Learnings from STARC-SUD Implementation
The implementation of STARC-SUD across different metropolitan regions offered valuable insights into the practical realities of delivering a culturally adapted group intervention to refugees with hazardous substance use. These learnings concern recruitment, engagement, linguistic mediation, group dynamics, and the development of therapeutic relationships. Recruitment proved much more difficult than anticipated. The rapid assessment underlying PREPARE showed that refugees who misuse substances form a particularly hard-to-reach group, partly because of fears about legal consequences, stigma and mistrust of institutions (Hertner et al., 2023). Outreach through shelters was often ineffective, while approaches through trusted community members and informal networks were more promising (Hertner et al., 2023). Unstable living conditions, frequent relocations and the stressful realities of asylum procedures further reduced predictability for participants.
Engagement and retention required flexibility and adaptation. Pilot groups and focus-group feedback highlighted that participants sometimes found conventional psychotherapy practices unfamiliar. Some preferred direct and activity-oriented sessions over ice-breaker exercises, while others needed culturally familiar emotion-regulation strategies rather than relaxation techniques that felt foreign (Lotzin et al., 2021). Retention was strongly influenced by daily stressors, with scheduling flexibility and active follow-up proving essential.
Working with interpreters required particular attention. Emotion-regulation concepts did not always translate easily, and metaphors or idioms sometimes led to confusion when interpreters were unprepared (Lotzin et al., 2021). Pre-session briefings, simplified language, and adjustments to pace helped maintain fidelity.
Group composition and logistics posed recurring challenges. Cultural norms influenced how openly men were willing to discuss emotions, and practical barriers such as room availability, shared accommodation, and competing obligations led to fluctuating attendance. Ensuring gender- and language-appropriate groups and close cooperation with local services supported smoother delivery.
The therapeutic alliance across cultural boundaries became a central success factor. Many participants initially approached the program with skepticism, associating therapy with stigma or weakness. Clear explanations, acknowledgment of cultural norms around honor and masculinity, and a respectful atmosphere fostered trust and encouraged sustained participation.
In later stages of the project, social media became an increasingly important complementary recruitment tool. Short reels in Arabic, Farsi, and other relevant languages were developed to reach refugees outside formal settings. A key lesson was that translation alone was insufficient; each clip required culturally acceptable visual cues, platform-appropriate communication styles, and presenters perceived as authentic by the target group (Figure 2). Metrics such as views, follower increases, and engagement (comments, direct messages) indicated moderate reach through organic posting, while paid promotion produced a noticeable increase in visibility. However, it was not possible to determine a precise “conversion rate,” since most participants reported learning about STARC-SUD through combined channels (flyers, direct contact, and social media). Early monitoring suggests that the expanded campaign may have reached additional subgroups not accessed through traditional recruitment.

These process learnings underscore that implementing STARC-SUD requires more than manualized delivery. Effective outreach, flexible engagement strategies, careful linguistic mediation, sensitivity to group dynamics and strong therapeutic alliances are essential contributors to feasibility.
Sucht-und-Flucht.de – A Cross-Project Resource Hub on Addiction and Forced Migration (www.sucht-und-flucht.de)
Within the PREPARE consortium, the platform Sucht-und-Flucht.de was developed as a national, web-based resource hub dedicated to the intersection of substance use and forced migration. The platform is developed at the Center for Interdisciplinary Addiction Research (ZIS) at the University Medical Center Hamburg-Eppendorf (UKE) and hosted at the German Centre for Addiction Issues (DHS). Its purpose is to function as an online resource center that disseminates findings, tools, and good-practice materials generated across the different subprojects of the consortium during its funding period. The platform is aimed at researchers, counsellors, therapists, and frontline workers involved in refugee support and addiction services.
Throughout the project, written and audiovisual materials relevant to practitioners were systematically collected, curated, and bibliographically documented. These include psychoeducational brochures, practice-oriented guides, and psychometric screening instruments in languages frequently used by refugees in Germany. Initial efforts focused on Arabic, Farsi/Dari, Kurdish, and Tigrinya. As new displacement contexts emerged – particularly the arrival of refugees from Ukraine in 2022 – the platform was expanded to include Ukrainian and Russian resources, ensuring that the materials remained aligned with current needs.
Sucht-und-Flucht.de also serves as a continuously updated dissemination interface for the PREPARE consortium. Each of the subprojects contributes summaries of current activities, methodological developments, training materials, and newly published articles. In addition, the platform functions as a repository for culturally adapted instruments and practice examples developed in PREPARE, facilitating access for practitioners nationwide. By integrating outputs from all subprojects, the website provides a coherent, interdisciplinary, and multilingual knowledge base that supports evidence-based work with refugees affected by substance use.
The establishment of Sucht-und-Flucht.de reflects PREPARE’s commitment to sustainable knowledge translation. Beyond presenting academic results, the platform enables direct transfer into practice and public health, ensuring that the insights developed during the project remain accessible and useful to professionals across Germany and internationally. It is not a static publication but a dynamic, evolving digital resource (Figure 3).
Integrating Learnings Across PREPARE
Synergies Between Subprojects
From the outset, the PREPARE consortium was designed so that its subprojects would mutually inform each other rather than operate in isolation. The rapid assessment (TP1) provided the foundational empirical insights into patterns of substance use among refugees, highlighting which groups were especially affected and which barriers shaped access to care. Qualitative and quantitative findings consistently showed that refugees who use alcohol or drugs were exceptionally difficult to reach due to fear of legal consequences, stigma, and low levels of trust toward formal services. Many lived in collective accommodation where insecurity, lack of privacy, overcrowding, and administrative pressure contributed to both psychological distress and elevated risk of substance use (Hertner et al., 2023). These findings strongly shaped the design of TP4 (STARC-SUD), which adopted outreach strategies grounded in personal contact, community trust, cultural mediation, and flexible scheduling.
At the same time, TP2, which focused on the translation and cultural adaptation of screening and assessment tools, provided essential methodological support for the wider PREPARE program. Many established diagnostic instruments were linguistically or conceptually unsuitable for refugees, requiring careful adaptation to Arabic and Farsi/Dari, including simplified wording and culturally meaningful symptom phrasing. The resulting instruments, based on a systematic review of available translations and their psychometric properties, were disseminated via the Sucht-und-Flucht.de platform, providing broader access for practitioners across Germany. Thus, TP2 directly contributed to strengthening diagnostic capacity within and beyond PREPARE.
The work of TP4 itself was influenced by insights from both TP1 and TP2. The emotion-regulation-based intervention was shaped by TP1 findings on stressors specific to refugee life – such as disrupted sleep, noise, bureaucratic pressure, and social isolation – and by TP2’s diagnostic work, which made it possible to screen participants in culturally appropriate ways. Additionally, TP4’s iterative adaptation process benefited from PREPARE’s broader knowledge-sharing structure, in which experiences from fieldwork, assessment, therapeutic delivery, and recruitment were continuously discussed across sites and disciplines.
The Sucht-und-Flucht platform integrates outputs from all subprojects into a shared national resource, facilitating cross-project exchange and access to key materials for practitioners, policymakers, and researchers.
Insights for Future Multi-Site Refugee SUD Projects
The PREPARE consortium offers several important lessons for designing and scaling multi-site interventions addressing substance use among refugees. One of the clearest insights is that robust baseline data are indispensable. Findings from the rapid assessment demonstrated that patterns of substance use vary considerably between sites and subgroups, and that stigma, fear of legal consequences, and structural barriers strongly inhibit participation. These realities highlight that multi-site projects must adapt recruitment strategies, outreach channels, and intervention framing to local conditions rather than assuming uniform applicability (Hertner et al., 2023).
A second lesson concerns the value of openly accessible, culturally adapted tools. PREPARE’s work on translating and validating screening instruments showed that reliable assessment across sites requires language-appropriate and culturally meaningful measures. By making these tools publicly available through the Sucht-und-Flucht platform, the consortium created a shared diagnostic basis that can be immediately used by practitioners in different regions. This reduces entry barriers for future projects and allows harmonized assessment across settings.
Third, PREPARE demonstrated that centralized dissemination infrastructures support both feasibility and long-term sustainability. The Sucht-und-Flucht platform evolved into a national hub for practice materials, diagnostic instruments, and project outputs. It was continuously updated with new languages, tools, and summaries of ongoing activities, enabling knowledge transfer beyond PREPARE’s internal network. Because the platform pools materials from multiple subprojects, it allows new initiatives to build directly on existing resources rather than starting from scratch.
A further consideration concerns the technical sustainability of the Sucht-und-Flucht platform itself. Through the recent upgrade of its content-management system, the platform is now secured for reliable, low-cost operation until at least 2029, supported by an affordable annual maintenance option offered by the hosting provider. At the same time, the upgrade ensures that the system can be smoothly updated to future versions and adapted to new devices, browsers, and accessibility standards well into the 2030s. For future multi-site refugee SUD projects, such long-term digital planning – both technically and financially – should be integrated from the very beginning to safeguard essential infrastructure and avoid costly redevelopment later on.
Additionally, PREPARE illustrates the importance of integrated workflows. Insights from needs assessment (TP1), diagnostic adaptation (TP2), and intervention development (TP4) reinforced one another and contributed to implementation strategies that were more culturally sensitive, realistic, and site-responsive. For future multi-site refugee SUD projects, such integrative structures – where data, tools, interventions, and dissemination mechanisms are interconnected – will be essential for achieving scalability without compromising contextual fit. Finally, future projects should consider the specific needs of migrants in transit. In contexts with heightened mobility, interventions that span several sessions may not be feasible, and more research is needed to understand how the barrier to adequate care can be overcome under these particular circumstances.
PREPARE shows that multi-site SUD interventions for refugees can be scaled effectively when projects build on high-quality local data, accessible diagnostic tools, robust dissemination platforms and long-term technical planning.
Implications for European Policy and Practice
The PREPARE program demonstrates that addiction care systems across Europe must integrate the specific circumstances of refugees if they aim to provide effective and equitable services. The rapid assessment conducted in TP1 showed that systematic data on substance use among refugees are largely absent. It identified which groups are particularly affected, which substances are used, and what environmental and structural factors influence consumption and help-seeking. Such baseline information is essential for meaningful policy development: without it, national and European decision-makers cannot allocate resources effectively or monitor intervention outcomes (Hertner et al., 2023). European member states could benefit from coordinated monitoring systems that collect comparable data across countries, allowing refugee-related substance-use trends to be understood more systematically.
A further central insight from PREPARE is the necessity of cultural and linguistic adaptation. TP2 demonstrated that existing screening instruments often fail to capture the needs and experiences of refugees because they rely on unfamiliar terminology, unvalidated translations, or culturally inappropriate symptom descriptions. By adapting tools such as the AUDIT and DUDIT to Arabic and Farsi/Dari, PREPARE showed how reliable assessment becomes possible when language and cultural context are taken seriously. European addiction-care frameworks should therefore emphasize investment in multilingual assessment tools, interpreter services, and cultural mediators to prevent misdiagnosis and exclusion.
In addition, PREPARE highlights the importance of integrated mental-health and substance-use care. Refugees often experience trauma, uncertainty, and daily stressors alongside hazardous alcohol or drug use. Separate treatment pathways for mental health and addiction, common in many European systems, can therefore be difficult to navigate and may fragment care. TP4’s emotion-regulation-based approach illustrates how linking trauma-related stress with substance-use mechanisms can create interventions that reflect refugees’ lived experiences (Lotzin et al., 2021). European policymakers could support integrated care pathways that merge trauma-informed and addiction-focused approaches instead of treating them as separate domains.
The Sucht-und-Flucht.de platform further demonstrates PREPARE’s commitment to sustainable knowledge transfer. As a national repository of multilingual practice materials, adapted diagnostic tools, and project outputs, it provides practitioners across Germany — and potentially Europe — with direct access to evidence-based resources. European initiatives could replicate this model by funding similar centralized hubs for refugee-specific materials, strengthening cross-country knowledge exchange and reducing duplication of work.
Finally, PREPARE underscores the need for targeted engagement and outreach strategies. Refugees who use substances face stigma, legal insecurity, and distrust of formal institutions, making them difficult to reach through standard services. Effective outreach requires collaboration with trusted community members, culturally resonant communication, and flexible scheduling. Psychoeducation that normalizes help-seeking and explains the purpose of services also plays a critical role. European policy could support these approaches by funding training programs for cultural mediators, outreach teams in refugee shelters, and low-threshold access points for addiction care.
Overall, PREPARE calls for addiction-care systems across Europe to adopt a data-informed, culturally sensitive, integrated, and sustainable approach. Investing in culturally adapted tools, integrated treatment models, accessible digital platforms, and long-term planning can enable more inclusive and effective responses to substance use among refugees.
Conclusion
The PREPARE consortium has filled a gap in the understanding of substance use among refugees in Germany. By combining empirical needs assessment, culturally adapted diagnostic tools, and an emotion-regulation–based intervention, the network demonstrated how different methodological strands can reinforce one another and produce a more accurate and practice-relevant picture of the challenges faced by displaced populations. The rapid assessment highlighted structural and contextual barriers to care, while the development of multilingual instruments enabled more reliable identification of individuals with hazardous substance use. STARC-SUD, as the therapeutic component of the program, showed the potential of interventions that link emotion regulation with substance-use behavior—an approach that aligns well with the psychological realities of many refugees.
Across all subprojects, PREPARE revealed that reaching refugees with substance-related problems requires persistent engagement, cultural sensitivity, and strong cooperation with community actors. Many of the barriers encountered in the recruitment and implementation phases reflect broader structural issues that will not be resolved by single interventions alone. At the same time, PREPARE’s outputs — particularly the Sucht-und-Flucht platform — illustrate how digital infrastructures can support practitioners by providing accessible, multilingual materials, diagnostic tools, and summaries of project activities.
Looking forward, the lessons from PREPARE point to the need for long-term, multi-level strategies within European addiction-care systems. These include sustained data collection, culturally informed diagnostics, integrated mental health and substance use treatment, and the development of digital tools that make knowledge widely available. By strengthening these components, health systems can respond more effectively to the needs of refugees and build the foundations for more inclusive and responsive addiction care across Europe.
Ethical approval
This study was approved by the Ethics Committee of the Medical Association Hamburg (Ethik-Kommission der Ärztekammer Hamburg) (Date: December 2, 2019, Decision/Protocol No: PV7132). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study was supported by the German Federal Ministry of Education and Research (BMBF) under Grant Number 01EF1805A-E.
Generative AI statement
The authors declare that during the preparation of this publication, the following AI-assisted technology was used: ChatGPT (OpenAI) on 01/11/2025 – 28/11/2025. Extent of Use: ChatGPT (OpenAI) was used occasionally for language editing and sentence-level refinement, particularly to improve clarity and conciseness (e.g., shortening sentences in the abstract). The tool was not used for data analysis, interpretation of results, or generation of scientific content. All content was written, critically reviewed, and approved by the authors. The authors confirm that they have critically reviewed and edited any AI-generated content and take full responsibility for the integrity, accuracy, and originality of the publication. The authors certify that the original human contribution is maintained and that AI-assisted tools are not listed or cited as authors.
References
- Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217-237. https://doi.org/10.1016/j.cpr.2009.11.004
- Aleer, E., Alam, K., Rashid, A., Mohsin, M., & Eacersall, D. (2023). Substance abuse amongst refugee youth: A scoping review. Current Addiction Reports, 10(3), 594-609. https://doi.org/10.1007/s40429-023-00502-6
- Bernal, G., Jiménez-Chafey, M. I., & Domenech Rodríguez, M. M. (2009). Cultural adaptation of treatments: A resource for considering culture in evidence-based practice. Professional Psychology: Research and Practice, 40(4), 361-368. https://doi.org/10.1037/a0016401
- Blackmore, R., Boyle, J. A., Fazel, M., Ranasinha, S., Gray, K. M., Fitzgerald, G., Misso, M., & Gibson-Helm, M. (2020). The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLOS Medicine, 17(9), e1003337. https://doi.org/10.1371/journal.pmed.1003337
- Boettcher, V. S., Nowak, A. C., & Neuner, F. (2021). Mental health service utilization and perceived barriers to treatment among adult refugees in Germany. European Journal of Psychotraumatology, 12(1), 1910407. https://doi.org/10.1080/20008198.2021.1910407
- Chen, W., Hall, B. J., Ling, L., & Renzaho, A. M. (2017). Pre-migration and post-migration factors associated with mental health in humanitarian migrants in Australia and the moderation effect of post-migration stressors: Findings from the first wave data of the BNLA cohort study. Lancet Psychiatry, 4(3), 218-229. https://doi.org/10.1016/S2215-0366(17)30032-9
- Council of Europe. (2019). Supporting Young Refugees in Transition to Adulthood. Recommendation CM/Rec(2019)4 adopted by the Committee of Ministers of the Council of Europe on 24 April 2019. Retrieved August 15, 2025 from https://rm.coe.int/recommendation-cm-2019-4-supporting-young-refugees-transition-adulthoo/168098e814
- Devillé, W., Greacen, T., Bogic, M., Dauvrin, M., Dias, S., Gaddini, A., Jensen, N. K., Karamanidou, C., Kluge, U., Mertaniemi, R., i Riera, R. P., Sárváry, A., Soares, J. J. F., Stankunas, M., Straßmayr, C., Welbel, M., & Priebe, S. (2011). Health care for immigrants in Europe: Is there still consensus among country experts about principles of good practice? A Delphi study. BMC Public Health, 11(1), 699. https://doi.org/10.1186/1471-2458-11-699
- Dumke, L., & Neuner, F. (2023). Othering refugees: Psychotherapists’ attitudes toward patients with and without a refugee background. Psychotherapy Research, 33(5), 654-668. https://doi.org/10.1080/10503307.2022.2150097
- Ezard, N. (2012). Substance use among populations displaced by conflict: A literature review. Disasters, 36(3), 533-557. https://doi.org/10.1111/j.1467-7717.2011.01261.x
- Garcia, M. F., & Birman, D. (2022). Understanding the migration experience of unaccompanied youth: A review of the literature. American Journal of Orthopsychiatry, 92(1), 79-102. https://doi.org/10.1037/ort0000588
- Hajak, V. L., Sardana, S., Verdeli, H., & Grimm, S. (2021). A systematic review of factors affecting mental health and well-being of asylum seekers and refugees in Germany. Frontiers in Psychiatry, 12, 643704. https://doi.org/10.3389/fpsyt.2021.643704
- Heim, E., & Kohrt, B. A. (2019). Cultural adaptation of scalable psychological interventions: A new conceptual framework. Clinical Psychology in Europe, 1(4). https://doi.org/10.32872/cpe.v1i4.37679
- Hertner, L., Stylianopoulos, P., Heinz, A., Kluge, U., Schafer, I., & Penka, S. (2023). Substance (mis)use among refugees as a matter of social ecology: Insights into a multi-site rapid assessment in Germany. Conflict and Health, 17(1), 1. https://doi.org/10.1186/s13031-023-00499-9
- Kiselev, N., Pfaltz, M., Haas, F., Schick, M., Kappen, M., Sijbrandij, M., De Graaff, A. M., Bird, M., Hansen, P., Ventevogel, P., Fuhr, D. C., Schnyder, U., & Morina, N. (2020). Structural and socio-cultural barriers to accessing mental healthcare among Syrian refugees and asylum seekers in Switzerland. European Journal of Psychotraumatology, 11(1), 1717825. https://doi.org/10.1080/20008198.2020.1717825
- Koch, T., & Liedl, A. (2019). STARK: Skills-Training zur Affektregulation – ein kultursensibler Ansatz. Therapiemanual für Menschen mit Flucht- und Migrationshintergrund. Klett-Cotta.
- Koch, T., Ehring, T., & Liedl, A. (2020). Effectiveness of a transdiagnostic group intervention to enhance emotion regulation in young Afghan refugees: A pilot randomized controlled study. Behaviour Research and Therapy, 132, 103689. https://doi.org/10.1016/j.brat.2020.103689
- Kuhn, S., Zurhold, H., Lehmann, K., & Verthein, U. (2018). Drogenkonsum und Hilfebedarfe von Geflüchteten in Deutschland [Drug use and special needs of refugees in Germany]. Suchttherapie, 19(03), 140-147. https://doi.org/10.1055/a-0637-8126
- Leicht, A., & Köhnlein, R. (2018). „Niemanden zurücklassen“ – migrierte Menschen in der Drogen- und Suchthilfe [“Leaving no one behind” – Migrants in drug helping systems]. Suchttherapie, 19(03), 119-125. https://doi.org/10.1055/a-0618-1411
- Lems, A., Oester, K., & Strasser, S. (2020). Children of the crisis: Ethnographic perspectives on unaccompanied refugee youth in and en route to Europe. Journal of Ethnic and Migration Studies, 46(2), 315-335. https://doi.org/10.1080/1369183X.2019.1584697
- Lindert, J., Neuendorf, U., Natan, M., & Schäfer, I. (2021). Escaping the past and living in the present: A qualitative exploration of substance use among Syrian male refugees in Germany. Conflict and Health, 15(1), 26. https://doi.org/10.1186/s13031-021-00352-x
- Lopez-Atanes, M., Rosenkranz, M., Erkoreka, L., Recio-Barbero, M., Bari, M., Hiller, P., Penka, S., Lindert, J., Martens, M., & Schafer, I. (2025). Special needs of refugees with substance use disorders from conflict-affected countries: A comparison with German-born individuals. Social Psychiatry and Psychiatric Epidemiology, 60(7), 1563-1572. https://doi.org/10.1007/s00127-025-02842-2
- Lotzin, A., Lindert, J., Koch, T., Liedl, A., & Schafer, I. (2021). STARC-SUD - adaptation of a transdiagnostic intervention for refugees with substance use disorders [Special issue]. Clinical Psychology in Europe, 3, e5329. https://doi.org/10.32872/cpe.5329
- Müller-Funk, L., Üstübici, A., & Belloni, M. (2023). Daring to aspire: Theorising aspirations in contexts of displacement and highly constrained mobility. Journal of Ethnic and Migration Studies, 49(15), 3816-3835. https://doi.org/10.1080/1369183X.2023.2208291
- Nguyen, T. P., Al Asaad, M., Sena, M., & Slewa-Younan, S. (2024). Loneliness and social isolation amongst refugees resettled in high-income countries: A systematic review. Social Science & Medicine, 360, 117340. https://doi.org/10.1016/j.socscimed.2024.117340
- Penka, S. (2004). Migration und Sucht: Notwendigkeit einer “interkulturellen Selbsthilfe”? Leipziger Universitätsverlag. https://books.google.de/books?id=21HGAAAAIAAJ
- Penka, S., Faißt, H., Vardar, A., Borde, T., Mösko, M., Dingoyan, D., Schulz, H., Koch, U., Kluge, U., & Heinz, A. (2015). Der Stand der interkulturellen Öffnung in der psychosozialen Versorgung- Ergebnisse einer Studie in einem innerstädtischen Berliner Bezirk. Psychotherapie - Psychosomatik - Medizinische Psychologie, 65, 353-362. https://doi.org/10.1055/s-0035-1549961
- Penka, S., Schouler-Ocak, M., Heinz, A., & Kluge, U. (2012). Interkulturelle Aspekte der Interaktion und Kommunikation im psychiatrisch/psychotherapeutischen Behandlungssetting. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz, 55(9), 1168–1175. https://doi.org/10.1007/s00103-012-1538-8
- Pfeiffer, E., Behrendt, M., Adeyinka, S., Devlieger, I., Rota, M., Uzureau, O., Verhaeghe, F., Lietaert, I., & Derluyn, I. (2022). Traumatic events, daily stressors and posttraumatic stress in unaccompanied young refugees during their flight: A longitudinal cross-country study. Child and Adolescent Psychiatry and Mental Health, 16(1), 26. https://doi.org/10.1186/s13034-022-00461-2
- Schäfer, I., Hiller, P., Milin, S., & Lotzin, A. (2022). A multicenter, randomized controlled trial to compare the effectiveness of STARC-SUD (Skills Training in Affect Regulation – a Culture-sensitive approach) versus treatment as usual in trauma-exposed refugees with substance use problems. Trials, 23(1), 915. https://doi.org/10.1186/s13063-022-06761-4
- Schwarzkopf, L., Künzel, J., Murawski, M., & Riemerschmid, C. (2023). Suchthilfe in Deutschland 2022. Jahresbericht der deutschen Suchthilfestatistik (DSHS). IFT Institut für Therapieforschung, München.
- Stylianopoulos, P., Hertner, L., Schäfer, I., Heinz, A., & Penka, S. (2023). Erleichterter Zugang zur ambulanten Suchthilfe für Geflüchtete. Sucht, 69(5), 224-234. https://doi.org/10.1024/0939-5911/a000833
- Sweeney, M. M., Rass, O., DiClemente, C., Schacht, R. L., Vo, H. T., Fishman, M. J., Leoutsakos, J.-M. S., Mintzer, M. Z., & Johnson, M. W. (2018). Working memory training for adolescents with cannabis use disorders: A randomized controlled trial. Journal of Child & Adolescent Substance Abuse, 27(4), 211-226. https://doi.org/10.1080/1067828X.2018.1451793
- Uzureau, O., Lietaert, I., Senovilla Hernández, D., & Derluyn, I. (2024). Multi-layered mobilities: Unaccompanied minors’ trajectories, decision-making and mobility after arrival in Italy. Children’s Geographies, 22(3), 431-446. https://doi.org/10.1080/14733285.2024.2302107
- van Dorp, M., Boon, A., Spijkerman, R., & Los, L. (2021). Substance use prevalence rates among migrant and native adolescents in Europe: A systematic review. Drug and Alcohol Review, 40(2), 325-339. https://doi.org/10.1111/dar.13154
- von Glahn-Middelmenne, C. (2023). Bericht 2023 des nationalen REITOX-Knotenpunkts an die EMCDDA. Workbook Treatment. Deutsche Hauptstelle für Suchtfragen (DHS).
- Weiss, N. H., Kiefer, R., Goncharenko, S., Raudales, A. M., Forkus, S. R., Schick, M. R., & Contractor, A. A. (2022). Emotion regulation and substance use: A meta-analysis. Drug and Alcohol Dependence, 230, 109131. https://doi.org/10.1016/j.drugalcdep.2021.109131
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.