Abstract
Refugee children and adolescents represent one of the most vulnerable populations in terms of health and psychosocial well-being due to exposure to war, forced displacement, family separation, poverty, discrimination, and acculturation-related stressors. This review aims to examine substance use among refugee adolescents within the context of migration from a public health perspective and to synthesize current empirical evidence on associated risk and protective factors. A systematic literature review of studies published between 2015 and 2024 was conducted using PubMed, Scopus, Web of Science, Google Scholar, and national Turkish databases. The review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. Eight empirical studies conducted in Türkiye, Australia, Sweden, Palestine, Jordan, and Serbia met the inclusion criteria. The findings indicate that, in a limited number of studies including direct comparisons, substance use among refugee adolescents tends to be higher than among their non-refugee peers. Tobacco use emerged as the most prevalent behavior, while alcohol and illicit substance use were more prominent in resettlement contexts characterized by acculturative stress. Key risk factors included trauma exposure, psychological distress, disrupted family functioning, peer influence, low socioeconomic status, and limited access to education and psychosocial support. Substance use frequently co-occurred with mental health problems such as anxiety, depression, and post-traumatic stress disorder, increasing vulnerability to violence, victimization, and other high-risk behaviors. Conversely, school connectedness, supportive family relationships, and social support networks functioned as important protective factors. Overall, the findings suggest that substance use among refugee adolescents should be conceptualized as a multidimensional public health concern shaped by the interaction of developmental sensitivity and displacement-related adversity. Culturally sensitive, community-based prevention and intervention strategies targeting refugee adolescents are urgently needed.
Keywords: refugee adolescents, migration, substance use, public health, addiction risk, systematic review
Main Points
- Refugee adolescents show elevated substance use risk compared to non-refugee peers in studies with direct comparisons.
- Tobacco use is the most prevalent behavior, while alcohol and illicit substance use vary across migration contexts.
- Substance use is strongly associated with trauma exposure, psychological distress, and socioeconomic disadvantage.
- Family dynamics and peer influences are key determinants of substance use behaviors.
- School connectedness and social support act as important protective factors.
Introduction
Forced displacement has reached unprecedented levels globally, driven by escalating armed conflicts and sociopolitical instability. These conditions continue to uproot millions of individuals every year, including large numbers of children and adolescents who are disproportionately affected by the consequences of forced migration (Güntay, 2023; Özaslan, 2023). According to the United Nations, a refugee is defined as “a person who, owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group, or political opinion, is outside the country of his nationality and is unable or unwilling to return” (United Nations High Commissioner for Refugees [UNHCR], 2018). Beyond the immediate act of relocation, refugees must navigate significant social, economic, cultural, and psychological challenges that complicate settlement and adaptation in host countries (Akgün, 2023).
Migration is therefore not merely the movement of individuals across borders but a complex public health phenomenon with profound implications for physical, mental, and social well-being. During the pre-migration and transit phases, refugees are often exposed to insecurity, trauma, infectious diseases, malnutrition, and disruptions in access to essential services (Daher et al., 2021; Morales-Muñoz et al., 2020). Following resettlement, socioeconomic deprivation (Gollopeni, 2020), educational discontinuity (Akgün, 2023), and cultural adaptation difficulties (Yaman, 2022) remain prevalent. According to the UNHCR Global Report, one in every seventy-four people worldwide has been forcibly displaced, and nearly half of this population consists of children and adolescents (UNHCR, 2022, 2023). These figures underscore that the health and well-being of refugee youth represent a critical dimension of global public health.
Adolescence is a developmental period marked by rapid biological, cognitive, and psychosocial change, during which individuals are particularly sensitive to environmental stressors (Alpaslan, 2012). Developmental tasks such as identity formation, increasing autonomy, and evolving peer relationships heighten emotional vulnerability. During this stage, adverse experiences associated with forced migration may disrupt key developmental processes, including identity formation, impulse control, emotional regulation, and executive functioning. As a result, mental health problems—including depression, anxiety, suicidal ideation, and substance use—frequently emerge or intensify during adolescence (Sharp et al., 2018). National data indicate that the average age of first substance use among the general youth population in Türkiye is approximately 15–17 years; however, nationally representative data specific to refugee adolescents are currently unavailable.
For refugee adolescents, the combined effects of war, forced migration, and ongoing stressors further amplify developmental risks. Evidence shows that traumatic experiences significantly increase vulnerability to anxiety disorders, adjustment problems, major depressive disorder (MDD), and post-traumatic stress disorder (PTSD), all of which are associated with heightened likelihood of substance use (Pfeiffer et al., 2022; Uygun et al., 2023). Additionally, persistent adversities such as discrimination, loss, and cultural alienation may lead adolescents to adopt maladaptive coping mechanisms, including substance use as a form of self-medication or psychological escape (Bilecik, 2019; Kara & Nazik, 2018; Vasic et al., 2021).
Given the increasing prevalence of substance use among refugee adolescents and the complex interplay between forced migration and adolescent development, a comprehensive and evidence-informed understanding of this issue is urgently needed. Existing reviews on refugee mental health have primarily focused on psychological problems such as depression, anxiety, and post-traumatic stress disorder, often treating substance use as a secondary outcome. Moreover, the interaction between migration-related stressors and adolescence-specific developmental vulnerabilities has received limited attention. This review addresses this gap by synthesizing empirical evidence on substance use among refugee adolescents from a public health and developmental perspective, thereby conceptualizing substance use as a multidimensional public health concern shaped by displacement-related adversity and developmental sensitivity.
Methods
Search Strategy
A systematic literature search was conducted in PubMed, Scopus, Web of Science, Google Scholar, and Turkish national databases (TR Dizin). The search covered all studies published between January 2015 and October 2024. Boolean operators were applied, and database-specific search strings were customized separately for each platform. Searches were performed between 28 and 31 October 2024 and included both English- and Turkish-language sources. A detailed list of all database-specific search strings, including the Turkish-language terms, is provided in Supplementary Table 1.
Eligibility Criteria
To enhance developmental precision and ensure methodological consistency, adolescence was defined as ages 10–19 years in accordance with the World Health Organization and UNICEF classifications. Studies were eligible for inclusion only if they reported data specifically for participants within this age range. Studies including mixed-age samples (e.g., participants younger than 10 years or older than 19 years) were included only when adolescent-specific data (10–19 years) could be clearly extracted from the results. Studies were excluded if age-disaggregated data for adolescents were not available, if the sample consisted exclusively of younger children or older youth/young adults, or if age groups were not clearly specified. This approach ensured that all included evidence directly pertained to adolescents within the intended developmental period.
Study Selection
All records retrieved from the database searches were imported into EndNote, and duplicate entries were removed before screening. The selection process was conducted by the single author of this review. To minimize potential selection bias, the author carried out the screening procedure twice at different times, first reviewing the titles and abstracts and then examining the full texts of potentially eligible studies. The reasons for excluding studies at the full-text stage were documented to ensure transparency and reproducibility.
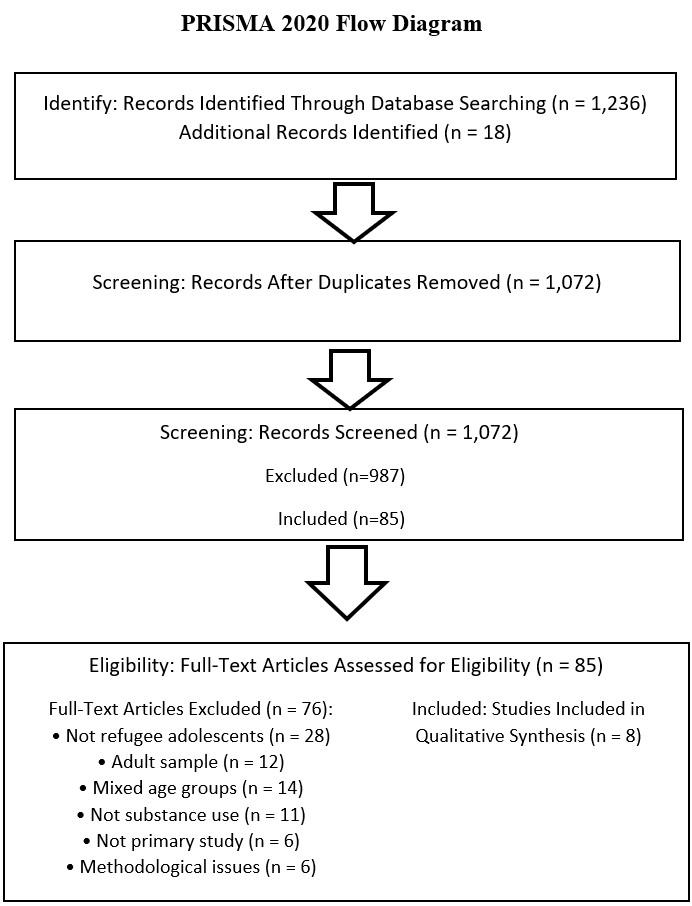
PRISMA Flow Diagram
The study selection process followed PRISMA 2020 guidelines. The complete PRISMA Flow Diagram is presented in Figure 1.
Risk of Bias Assessment
Risk of bias was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklists suitable for each study design: cross-sectional, qualitative, or cohort. Each study was evaluated across sampling adequacy, measurement validity, confounder control, clarity of data analysis, and outcome reliability. Studies were rated as low, moderate, or high risk of bias. A full summary is presented in Table 1.
| Table 1. Risk of Bias Assessment (JBI) | |||||||
| Study | Design | Sampling Adequacy | Measurement Validity | Confounder Control | Data Analysis Clarity | Outcome Reliability | Overall Bias |
| Kheirallah et al., 2020 | Cross-sectional | Moderate | Moderate | Moderate | Clear | Moderate | Moderate |
| Snoubar et al., 2023 | Cross-sectional | Moderate | Moderate | Low | Clear | Moderate | Moderate |
| Manhica et al., 2017 | Cohort | High | High | High | Clear | High | Low |
| Posselt et al., 2017 | Qualitative | High | High | N/A | Clear | High | Low |
| Hirani et al., 2018 | Cross-sectional | Moderate | Moderate | Low | Clear | Moderate | Moderate |
| İlhan et al., 2021 | Cross-sectional | Moderate | Moderate | Low | Clear | Moderate | Moderate |
| Vasic et al., 2021 | Cross-sectional | Moderate | Moderate | Low | Clear | Moderate | Moderate |
| Taylan & Barış, 2017 | Cross-sectional | Moderate | Low | Low | Moderate | Moderate | Moderate |
Ethical Considerations
As this study does not involve any human participants or primary data collection, ethical approval was not required. The research was conducted in accordance with general principles of research and publication ethics.
Results
Study Characteristics
A total of eight studies met the inclusion criteria. These studies were conducted in Türkiye (n = 2), Australia (n = 2), Sweden (n = 1), Palestine (n = 1), Jordan (n = 1), and Serbia (n = 1). Six studies used a cross-sectional design, one used a registry-based cohort design, and one employed a qualitative design. Sample sizes ranged from 48 to 1,159 adolescents, and all studies focused specifically on refugee adolescents aged 10–19 years, or provided adolescent-specific analyses. A detailed summary of study features is presented in Table 2.
| Table 2. Characteristics of the included studies | |||||||
| Authors (Year) | Country | Sample | Study Design | Substance Type | Key Measures | Key Findings | Risk of Bias |
| Kheirallah et al., 2020 | Jordan | 1,159 Syrian refugee adolescents 12-18 | Cross-sectional | Tobacco, waterpipe | Trauma exposure, PTSD, mental health, smoking patterns, social support | Trauma exposure and low social support significantly increased tobacco and waterpipe use; boys smoked more | Moderate |
| Snoubar et al., 2023 | Palestine | 427 Palestinian refugee adolescents aged 13–18 | Cross-sectional | High-risk drug use, tobacco, energy drinks | Substance use behaviors, socioeconomic stressors, peer influence, family stress | High-risk drug use linked to poverty, family stress, and peer influence; boys reported higher use | Moderate |
| Manhica et al., 2017 | Sweden | Young refugees arriving at ages 13–19 (national cohort) | Registry-based cohort | Alcohol-related disorders | Hospital admission records, migration age, follow-up data | Higher risks of alcohol-related admissions than native peers; risk varied by origin and migration age | Low |
| Posselt et al., 2017 | Australia | 48 refugee-background adolescents/youth (majority 15–19) | Qualitative (interviews, focus groups) | Alcohol, illicit drugs | Settlement stress, trauma, peer/family influence | Substance use as coping with trauma, discrimination, acculturation stress | Moderate |
| Hirani et al., 2018 | Australia | 233 refugee adolescents aged 12–19 | Cross-sectional | Cigarettes, alcohol, other substances | Psych distress, acculturative stress, family functioning, social support | Distress, acculturative stress, poor family functioning increased substance use | Moderate |
| İlhan et al., 2021 | Türkiye | 356 Syrian refugee adolescents aged 12–18 | Cross-sectional | Cigarettes, alcohol, volatile substances | Peer deviance, school connectedness, family conflict | Peer deviance and family conflict showed significant associations with substance use, while school connectedness was inversely associated with substance involvement. | Moderate |
| Vasic et al., 2021 | Serbia | 512 refugee/migrant adolescents aged 11–19 | Cross-sectional | Cigarettes, alcohol, marijuana | Trauma history, migration stress, family separation | Substance use associated with trauma, family separation; unaccompanied boys at higher risk | Moderate |
| Taylan & Barış, 2017 | Türkiye | 302 Syrian refugee adolescents aged 12–17 | Cross-sectional | Cigarettes, alcohol | Social integration, neighborhood safety, peer influence | Low social integration, unsafe neighborhoods increased substance use | Moderate |
Across the selected studies, tobacco use emerged as the most frequently reported substance-related behavior. Higher cigarette and waterpipe smoking rates were consistently observed among male adolescents, particularly in Middle Eastern contexts (İlhan et al., 2021; Kheirallah et al., 2020). Waterpipe use was notably prevalent among adolescents exposed to displacement-related trauma and living in resource-limited environments (Kheirallah et al., 2020). High-risk drug use was reported among Palestinian refugee adolescents residing in refugee camps, where socioeconomic stressors and peer influence played a central role (Snoubar et al., 2023). Alcohol-related health issues were also documented, with young refugees in Sweden experiencing significantly higher alcohol-related hospitalizations compared to native peers (Manhica et al., 2017). Patterns of illicit drug use, though less frequently measured, were more common among unaccompanied boys and adolescents exposed to prolonged migration stress or insecure housing arrangements (Vasic et al., 2021).
Several interrelated risk factors contributed to substance use among refugee adolescents. Exposure to war-related trauma and psychological distress was frequently linked with tobacco, alcohol, and drug use, suggesting that substances were sometimes used as maladaptive coping strategies (Hirani et al., 2018; Snoubar et al., 2023; Vasic et al., 2021). This was further supported by qualitative findings that identified coping with trauma, discrimination, and acculturative stress as primary drivers of substance use in resettled youth (Posselt et al., 2017). Acculturative stress, social isolation, and perceived discrimination were also associated with increased risk of substance use, particularly in settings where adolescents struggled with integration challenges (Hirani et al., 2018).
Family-related determinants were prominent across the studies. Low parental monitoring, family conflict, and weakened family cohesion were consistently associated with a higher likelihood of substance use (Hirani et al., 2018; İlhan et al., 2021). Peer influence emerged as one of the strongest predictors of substance use; adolescents with substance-using or deviant peers demonstrated substantially elevated risk (İlhan et al., 2021; Snoubar et al., 2023). Environmental factors, including unsafe neighborhoods, overcrowded living conditions, and limited access to structured recreational activities, further heightened vulnerability to substance use among refugee adolescents (Taylan & Barış, 2017; Vasic et al., 2021).
Despite the range of identified risks, several protective factors were also documented. Strong parental monitoring, supportive family relationships, school connectedness, and structured educational environments were identified as critical buffers that reduced substance use risk (Hirani et al., 2018; İlhan et al., 2021). Additionally, social support networks and a sense of community belonging were reported as protective influences that enhanced resilience and discouraged substance use among adolescents adjusting to new environments (Hirani et al., 2018; Taylan & Barış, 2017).
Finally, the risk of bias assessment indicated that most cross-sectional studies exhibited moderate methodological limitations, primarily related to sampling procedures and limited control for confounders. In contrast, the cohort study conducted in Sweden demonstrated low risk of bias, and the qualitative study showed strong methodological rigor (Manhica et al., 2017; Posselt et al., 2017). Overall, evidence quality was considered acceptable, though findings should be interpreted with attention to the predominance of cross-sectional designs (Table 2).
Discussion
This systematic review synthesizes evidence from eight empirical studies conducted across diverse sociocultural and displacement contexts. The findings consistently demonstrate that substance use is associated with a constellation of psychosocial, environmental, and migration-related stressors. However, because most included studies employed cross-sectional designs, these relationships cannot be interpreted as causal and instead reflect co-occurring vulnerabilities that require longitudinal validation.
Across settings such as Türkiye, Jordan, Sweden, Australia, Palestine, and Serbia, tobacco use including cigarette and waterpipe smoking emerged as the most frequently documented behavior. Tobacco and waterpipe use were associated with trauma exposure, psychological distress, limited social support, and socioeconomic hardship. Alcohol-related harms were more prominent in high-income resettlement contexts, where acculturation difficulties and integration challenges were linked with higher levels of alcohol consumption. Although less commonly assessed, illicit drug use was related to family separation, unaccompanied minor status, and unstable living arrangements, highlighting the compounded risks faced by highly vulnerable subgroups.
Trauma exposure and daily stressors stemming from forced displacement were among the most pervasive correlates of substance use. Several studies reported that higher levels of trauma were associated with increased involvement in tobacco, alcohol, or drug use. Qualitative findings further suggested that substances may serve as maladaptive coping strategies for managing discrimination, loss, and acculturative tension; nonetheless, such interpretations remain speculative without temporal evidence. Only one longitudinal study (Pfeiffer et al., 2022) demonstrated that cumulative traumatic events and ongoing stressors may predict changes in mental health symptoms over time, which were subsequently linked with substance use. Despite this contribution, research directly examining predictive pathways to substance use among refugee adolescents remains limited.
Family and peer dynamics constituted another major domain influencing substance use. Weak parental monitoring, family conflict, and disrupted caregiving arrangements were strongly associated with higher substance use, whereas supportive family relationships and engaged parenting functioned as protective factors. Peer influences displayed similarly robust patterns: engagement with deviant, substance-using, or high-risk peer groups was consistently related to increased substance involvement. These findings align with developmental research indicating that peer affiliation becomes especially influential during adolescence—a process intensified in displacement contexts where social belonging is both urgently needed and difficult to secure.
Structural and environmental conditions further shaped vulnerability. Limited access to education, poverty, unsafe neighborhoods, and unstable housing were associated with elevated substance use. Unaccompanied minors were consistently identified as a high-risk subgroup; across studies, their substance use levels were linked with the absence of stable adult supervision, disrupted social environments, and heightened exposure to stress. These patterns underscore the intersection of developmental sensitivity, displacement-related adversity, and structural inequities.
Despite these risks, several protective mechanisms emerged. School connectedness, community belonging, structured recreational activities, and supportive peer relationships were associated with lower levels of substance use. These findings highlight the importance of strengthening multi-level protective systems tailored to adolescents’ developmental needs and displacement experiences.
Methodologically, the evidence base exhibited considerable heterogeneity. The reliance on cross-sectional designs and non-probability sampling limits both temporal interpretation and generalizability. Substantial variation in measurement tools, substance categories, and migration-related variables further complicates comparative analysis. Only one longitudinal and one qualitative study demonstrated stronger methodological rigor, underscoring an urgent need for more robust designs.
Taken together, the reviewed evidence suggests that substance use among refugee adolescents is associated with the cumulative interaction of trauma exposure, psychosocial distress, peer and family dynamics, and structural disadvantages. While consistent correlational patterns were identified, causal mechanisms cannot be inferred. Future research should prioritize longitudinal and mixed-methods approaches to clarify temporal pathways, examine developmental variations (early vs. middle vs. late adolescence), explore gender differences, and investigate mechanisms underlying substance use vulnerability, particularly among unaccompanied minors and adolescents living in camp-based or highly insecure environments.
Developmentally Sensitive Interpretation of Findings
Beyond these general patterns, integrating developmental science provides a more nuanced understanding of why substance use vulnerability varies across refugee adolescents. Adolescence encompasses distinct biological and psychosocial phases, and displacement-related hardship may intersect differently with each stage.
Early adolescents (10–13) experience heightened emotional reactivity and limited regulatory capacity, which may intensify the impact of trauma, family disruption, and environmental instability (Lustig et al., 2004; Steinberg, 2014). Middle adolescents (14–16), who show peak sensitivity to peer influence and social belonging (Somerville, 2013), may be particularly affected by deviant peer networks, consistent with findings linking peer deviance to substance use (İlhan et al., 2021; Snoubar et al., 2023). Late adolescents (17–19), undergoing identity exploration and autonomy seeking, may be more likely to experiment with alcohol and tobacco, especially in high-income host settings where substance availability and social exposure are greater (Patton et al., 2016).
Gender-specific pathways further shape vulnerability. Male refugee adolescents frequently demonstrate higher tobacco and substance use—patterns often linked to impulsivity and externalizing behaviors (Moffitt, 2018). Female adolescents may exhibit higher internalizing symptoms such as anxiety and depression (Vatansever & Erden, 2018), which could increase susceptibility to coping-related substance use. In addition, gender-based acculturative pressures—such as restrictions on girls’ mobility or expectations on boys to adopt host-country masculine norms—may reinforce distinct behavioral pathways (Hirani et al., 2018).
Pubertal timing represents another underexamined but influential factor. Early pubertal onset, associated with increased sensation seeking and greater responsiveness to peer influence, is a strong predictor of substance use across populations (Casey et al., 2016; Delevich et al., 2021). For refugee adolescents, chronic stress and adversity may alter pubertal trajectories (Felitti et al., 1998; Pfeiffer et al., 2022), potentially heightening risk. None of the included studies assessed pubertal timing, indicating an important gap for future research.
Finally, caregiving status distinguishes risk profiles across refugee youths. Unaccompanied minors—lacking parental monitoring and support—experience higher distress and more frequent substance use, consistent with prior research (Vasic et al., 2021). Accompanied adolescents generally benefit from emotional stability and supervision (Manhica et al., 2017), although these protective factors may diminish under camp or overcrowded living conditions.
Public Health Implications
The findings of this review point to several evidence-based public health implications. First, the consistent association between trauma, psychological distress, and substance use across multiple studies (e.g., Pfeiffer et al., 2022; Vatansever & Erden, 2018) highlights the need for trauma-informed mental health programs targeting refugee adolescents. Second, evidence showing that school connectedness is protective (İlhan et al., 2021; Snoubar et al, 2023) suggests that strengthening school engagement and retention should be a priority in prevention efforts. Third, studies identifying weakened parental monitoring and disrupted caregiving as risk factors (Manhica et al., 2017; Vasic et al., 2021) indicate that family-focused interventions may reduce substance use vulnerabilities.
Peer influence emerged as a strong correlate of substance use (İlhan et al., 2021; Snoubar et al, 2023), underscoring the need for programs that promote prosocial peer networks and safe community spaces. Additionally, evidence of heightened risk among unaccompanied minors (Vasic et al., 2021) supports prioritizing specialized services such as safe housing, mentorship programs, and tailored psychosocial support. Finally, structural determinants including poverty, unsafe neighborhoods, and unstable housing were associated with increased substance use involvement, emphasizing the importance of integrating public health strategies with broader social policies addressing social determinants of health.
Together, these implications call for multilevel interventions that address individual, family, peer, and environmental factors to reduce substance-related harms among refugee adolescents.
Conclusion
This review indicates that substance use among refugee adolescents is associated with multiple psychosocial, developmental, and structural factors across diverse displacement settings. Tobacco use was the most frequently reported behavior, while alcohol and illicit substance use appeared more prominently in resettlement contexts marked by acculturative stress. These patterns were consistently linked with trauma exposure, psychological distress, weakened family supervision, and deviant peer networks, whereas school connectedness and supportive relationships were associated with lower substance involvement.
Due to the predominance of cross-sectional designs, these relationships should not be interpreted as causal. Only one longitudinal study offered preliminary evidence that cumulative trauma may predict changes in mental health that are related to substance use. More rigorous longitudinal and mixed-methods studies are needed to clarify temporal pathways, developmental differences, and mechanisms of vulnerability, particularly among unaccompanied minors.
Overall, the findings of this review suggest that substance use among refugee adolescents should be conceptualized as a multidimensional public health concern shaped by displacement-related adversity and developmental sensitivity. It is recommended that prevention and intervention strategies be designed to strengthen protective systems and reduce risk in this highly vulnerable population. This review makes a unique and original contribution by integrating empirical evidence across diverse displacement contexts and highlighting the combined influence of trauma, psychosocial stressors, and structural vulnerabilities on substance use among refugee adolescents.
Limitations and Future Directions
Although this review provides a comprehensive synthesis of the literature on substance use among refugee adolescents, several limitations should be noted. Most included studies employed cross-sectional designs, limiting causal inference between risk factors and substance use behaviors. In addition, the evidence base is largely derived from high-income Western countries, whereas data from low- and middle-income host settings remain limited, constraining the generalizability of the findings.
Further limitations include substantial heterogeneity across studies in terms of refugee populations, migration contexts, age, gender, and cultural background, as well as the underrepresentation of female adolescents and inconsistent use of standardized measurement tools.
Future research should prioritize longitudinal and mixed-method approaches to better elucidate temporal pathways linking trauma exposure, acculturative stress, and substance use. Greater integration of biological, psychological, and sociocultural perspectives is needed, alongside intervention-based studies evaluating culturally adapted prevention and treatment programs. Strengthening cross-national research collaboration will be essential to inform evidence-based public health responses to substance use among refugee adolescents.
Author contributions
Conception and design: T.A.G.; Data acquisition: T.A.G.; Data analysis: T.A.G.; Data interpretation: T.A.G.; Drafting of the manuscript: T.A.G.; Critical revision of the manuscript: T.A.G. The author reviewed the results, approved the final version of the manuscript, and agreed to be accountable for all aspects of this study.
Data availability statement
Data sharing is not applicable to this article as no new datasets were generated or analyzed during this study.
Conflict of interest
The author declares that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author declares that this study received no funding.
Generative AI statement
The author declares that during the preparation of this study, the following AI-assisted technology was used: ChatGPT (OpenAI) on 2025–2026. Extent of Use: AI-assisted tools were used for language editing, grammar correction, and improving the clarity and readability of the manuscript. The author confirms that she has critically reviewed and edited any AI-generated content and takes full responsibility for the integrity, accuracy, and originality of the publication. The author certifies that the original human contribution is maintained and that AI-assisted tools are not listed or cited as authors.
References
- Akgün, A. (2023). A historical framework on the educational problems of migrant children in Turkey. Turkish Journal of Social Research, 27(2), 395-406. https://izlik.org/JA99JW24AK
- Alpaslan, A. H. (2012). Ergen ruh sağlığı ve spor. Kocatepe Tıp Dergisi, 13(3), 181-185. https://izlik.org/JA57TH62RW
- Bilecik, S. (2019). A quantitative study on the social skills of refugee children based on peer perceptions. Journal of Divinity Faculty of Hitit University, 18(35), 287-314. https://doi.org/10.14395/hititilahiyat.507178
- Casey, B. J., Galván, A., & Somerville, L. H. (2016). Beyond simple models of adolescence to an integrated circuit-based account: A commentary. Developmental Cognitive Neuroscience, 17, 128-130. https://doi.org/10.1016/j.dcn.2015.12.006
- Daher, B., Hamie, S., Pappas, K., Karim, M. N., & Thomas, T. (2021). Toward resilient water-energy-food systems under shocks: Understanding the impact of migration, pandemics, and natural disasters. Sustainability, 13(16), 9402. https://doi.org/10.3390/su13169402
- Delevich, K., Klinger, M., Okada, N. J., & Wilbrecht, L. (2021). Coming of age in the frontal cortex: The role of puberty in cortical maturation. Seminars in Cell & Developmental Biology, 118, 64-72. https://doi.org/10.1016/j.semcdb.2021.04.021
- Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245-258. https://doi.org/10.1016/s0749-3797(98)00017-8
- Gollopeni, B. (2020). Socio-economic situation of Kosovan migrants before and after migration. Traektoriâ Nauki, 6(10), 3001-3009. https://doi.org/10.22178/pos.63-7
- Güntay, N. (2023). Analyzing the new war concept within the context of the September 11 attacks and terrorism. Fırat University Journal of Social Sciences, 33(2), 889-905. https://doi.org/10.18069/firatsbed.1079596
- Hirani, K., Cherian, S., Mutch, R., & Payne, D. N. (2018). Identification of health risk behaviours among adolescent refugees resettling in Western Australia. Archives of Disease in Childhood, 103(3), 240-246. https://doi.org/10.1136/archdischild-2017-313451
- İlhan, M. N., Ekmekçi Ertek, İ., Gözükara, M. G., Akıl, Ö., Ursu, P., Ergüder, T., Polat, S., Şimşek, M. Y., Aktaş, M., Gazanfer, Ö. B., Özger İlhan, S., & Kaptan, H. (2021). Substance use in refugee camps and local community: Şanlıurfa sample. Archives of Neuropsychiatry, 58, 121-127. https://doi.org/10.29399/npa.24856
- Kara, P., & Nazik, E. (2018). Effect of migration on women and children’s health. Gümüşhane University Journal of Health Sciences, 7(2), 58-69. https://dergipark.org.tr/en/download/article-file/505816
- Kheirallah, K. A., Cobb, C. O., Alsulaiman, J. W., Alzoubi, A. H., Kana’an, H., & Mzayek, F. (2020). Trauma exposure, mental health and tobacco use among vulnerable Syrian refugee youth in Jordan. Journal of Public Health, 42(3), e343-e351. https://doi.org/10.1093/pubmed/fdz128
- Lustig, S. L., Kia-Keating, M., & Knight, W. G. (2004). Review of child and adolescent refugee mental health. Journal of the American Academy of Child & Adolescent Psychiatry, 43(1), 24-36. https://doi.org/10.1097/00004583-200401000-00012
- Manhica, H., Gauffin, K., Almquist, Y. B., Rostila, M., Berg, L., Rodríguez García de Cortázar, A., & Hjern, A. (2017). Hospital admissions due to alcohol-related disorders among young adult refugees who arrived in Sweden as teenagers: A national cohort study. BMC Public Health, 17, 644. https://doi.org/10.1186/s12889-017-4645-5
- Moffitt, T. E. (2018). Male antisocial behaviour in adolescence and adulthood: Developmental trends and explanations. Nature Human Behaviour, 2, 177-186. https://doi.org/10.1038/s41562-018-0309-4
- Morales-Muñoz, H., Jha, S., Bonatti, M., Alff, H., Kurtenbach, S., & Sieber, S. (2020). Exploring connections—environmental change, food security and violence as drivers of migration—a critical review of research. Sustainability, 12(14), 5702. https://doi.org/10.3390/su12145702
- Özaslan, K. (2023). Dış’tan iç’e evrilen bir kitlesel göç: Türkiye’nin Suriyelileri. Akademik Yaklaşımlar Dergisi, 14(1), 115-143. https://doi.org/10.54688/ayd.1279581
- Patton, G. C., Sawyer, S. M., Santelli, J. S., Ross, D. A., Afifi, R., Allen, N. B., Arora, M., Azzopardi, P., Baldwin, W., Bonell, C., Kakuma, R., Kennedy, E., Mahon, J., McGovern, T., Mokdad, A. H., Patel, V., Petroni, S., Reavley, N., Taiwo, K., …Viner, R. M. (2016). Our future: A Lancet commission on adolescent health and wellbeing. The Lancet, 387(10036), 2423-2478. https://doi.org/10.1016/S0140-6736(16)00579-1
- Pfeiffer, E., Behrendt, M., Adeyinka, S., Devlieger, I., Rota, M., Uzureau, O., Verhaeghe, F., Lietaert, I., & Derluyn, I. (2022). Traumatic events, daily stressors and posttraumatic stress in unaccompanied young refugees during their flight: A longitudinal cross-country study. Child and Adolescent Psychiatry and Mental Health, 16(1), 26. https://doi.org/10.1186/s13034-022-00461-2
- Posselt, M., McDonald, K., Procter, N., de Crespigny, C., & Galletly, C. (2017). Improving the provision of services to young people from refugee backgrounds with comorbid mental health and substance use problems: Addressing the barriers. BMC Public Health, 17(1), 280. https://doi.org/10.1186/s12889-017-4186-y
- Sharp, C., Vanwoerden, S., & Wall, K. (2018). Adolescence as a sensitive period for the development of personality disorder. Psychiatric Clinics of North America, 41(4), 669-683. https://doi.org/10.1016/j.psc.2018.07.004
- Snoubar, M., Kasim, S., Badawi, M., Shaban, Q., AbuAlrub, I., Hunjul, M., Khelfeh, N., Abuhassan, A., Hanani, A., Bilbeisi, S., & Damiri, B. (2023). High-risk drug use among Palestinian adolescent refugees in the North West Bank Palestine. Journal of Ethnicity in Substance Abuse, 24(1), 3-22. https://doi.org/10.1080/15332640.2023.2255850
- Somerville, L. H. (2013). The teenage brain: Sensitivity to social evaluation. Current Directions in Psychological Science, 22(2), 121-127. https://doi.org/10.1177/0963721413476512
- Steinberg, L. (2014). Age of opportunity: Lessons from the new science of adolescence. Houghton Mifflin Harcourt.
- Taylan, H. H., & Barış, İ. (2017, January). Göç sürecindeki Diyarbakır’da çocuklarda madde kullanım eğilimleri [Paper presentation]. Transnational Press London.
- United Nations High Commissioner for Refugees. (2018). 1951 Convention relating to the status of refugees and its 1967 Protocol: Definition of “refugee”. https://www.unhcr.org/about-unhcr/who-we-protect/refugees/
- United Nations High Commissioner for Refugees. (2022). Global report 2022. https://reporting.unhcr.org/global-report-2022
- United Nations High Commissioner for Refugees. (2023). Figures at a glance. https://www.unhcr.org/us/about-unhcr/who-we-are/figures-glance
- Uygun, S. D., Temeltürk, R. D., Efe, A., Canlı, M., Çetinkaya, M., & Çakmak, F. H. (2023). A retrospective analysis of the demographic and clinical characteristics of migrant children and adolescents. Journal of Adnan Menderes University Faculty of Health Sciences, 7(3), 662-673. https://doi.org/10.46237/amusbfd.1261530
- Vasic, J., Grujicic, R., Toskovic, O., & Pejovic Milovancevic, M. (2021). Mental health, alcohol and substance use of refugee youth. Frontiers in Psychiatry, 12, 713152. https://doi.org/10.3389/fpsyt.2021.713152
- Vatansever, M., & Erden, G. (2018). Mülteci çocuklar ve ergenler ile yapılan psikolojik görüşme üzerine bir derleme. Journal of Child and Adolescent Mental Health, 25(2), 175-186. https://cogepderg.com/tr/makaleler/multeci-cocuklar-ve-ergenler-ile-yapilan-psikolojik-gorusme-uzerine-bir-derleme/27691
- Yaman, F. (2022). The Euro-Turks’ sense of belonging and perceived othering scale: A validity and reliability study. İçtimaiyat: Journal of Social Sciences, 6, 213-228. https://doi.org/10.33709/ictimaiyat.1078440
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.