Abstract
This narrative review examines the efficacy and scope of prevention and therapy interventions for digital addiction among adolescents. Through a systematic analysis of peer-reviewed articles published between 2013 and 2023, this review identifies effective strategies and highlights research gaps. Cognitive behavioral therapy emerges as the predominant intervention, often incorporating parental involvement. However, limitations include small sample sizes, lack of long-term follow-up, and the absence of software-mediated therapies specifically designed for adolescents. The review also underscores the need for more diverse study populations, as existing research is concentrated in a few geographic regions. Future research should explore technology-based solutions tailored to adolescent needs and extend study durations to enhance treatment outcomes.
Keywords: addictions to technology, adolescents, cognitive behavioral therapy, diagnostic tests, internet addiction, treatment outcome
Main Points
- Cognitive behavioral therapy is the most commonly used and effective intervention for adolescent digital addiction.
- Parental involvement significantly enhances the success of intervention strategies.
- Long-term follow-up assessments are lacking in 40% of the reviewed studies, limiting the evaluation of sustained treatment effects.
- The absence of software-mediated interventions tailored to adolescents represents a significant research gap.
- Future research should explore interdisciplinary approaches and extend study durations to improve treatment outcomes.
Introduction
Digital addiction (DA) refers to an impulse control disorder related to obsessive and excessive use of digital devices, platforms, and technologies such as the internet, online platforms, video games, mobile devices, and social network platforms. It constitutes an emerging domain of Cyberpsychology (Singh & Singh, 2019).
The prevalence of digital devices nowadays has significantly influenced the behavioral patterns of adolescents, leading to increased concerns about DA. The prevalence of DA differs globally, varying between 8.90% in Eastern countries and 4.60% in Western countries (Pan et al., 2020); this discrepancy may be related to high demands for online activities and parenting attitudes toward Internet use (Griffiths et al., 2016). Recent studies indicate a rising trend in problematic digital media use among adolescents, with reports showing an increase from 7% in 2018 to 11% in 2022, highlighting the potential risks for developing problematic behaviors related to video games (World Health Organization, 2024). At present, Internet Gaming Disorder (IGD) is recognized in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) (American Psychiatric Association, 2013). While IGD is officially recognized in the DSM-5 as a diagnosable condition, DA remains a broader and less clearly defined concept encompassing excessive engagement with digital devices, social media, and online platforms beyond gaming (Kuss & Lopez-Fernandez, 2016). The absence of a universally accepted classification for DA leads to inconsistencies in diagnostic criteria, making it difficult to assess its true prevalence and to develop standardized intervention strategies (Brand et al., 2020). Some researchers categorized DA as a non-substance-related impulse control disorder marked by compulsive use of digital media, characterized by an inability to control the usage despite understanding its negative consequences (Harscoet et al., 2013; Imrani & Touri, 2025; Meskini et al., 2024; Shapira et al., 2003; Şimşek et al., 2019; Young, 1998).
Prior research has primarily focused on DA prevention and treatment programs, with less emphasis on tailored interventions for adolescents (Bağatarhan & Siyez, 2017; Cemiloglu et al., 2022). This gap highlights the need for a dedicated review of age-specific intervention strategies and their efficacy. This narrative review aims to systematically examine and evaluate preventive and therapeutic interventions for DA in adolescents, differentiating it from other reviews by the critical evaluation of intervention methodologies and focusing on types of DA examined and screening instruments used for adolescents.
The primary objective of this review is to explore and compare the various approaches implemented to combat DA among adolescents, assessing their effectiveness and identifying gaps in the existing literature. The review draws on peer-reviewed journals from 2013 to 2023 using a structured research strategy.
This review addresses a critical gap in literature by focusing exclusively on interventions targeting adolescents, a population undergoing major developmental transitions and particularly vulnerable to digital overuse. While previous reviews have examined DA in the general population or focused primarily on IGD, this study provides a dedicated synthesis of interventions designed for adolescents across a broad spectrum of digital behaviors. The originality of the present review lies in its structured comparison of prevention and treatment approaches, its analysis of age-appropriate screening tools, and its emphasis on contextual factors such as school, family, and clinical environments. The findings of this study have practical implications for educators, clinicians, and mental health professionals seeking evidence-based guidance on how to address digital overuse among adolescents. They also offer theoretical value by identifying trends, gaps, and typologies in intervention design and evaluation, which can help shape future research frameworks in this emerging field.
Conceptual Background
Digital addiction among adolescents is increasingly understood as a complex behavioral phenomenon situated at the intersection of self-regulation deficits, emotional vulnerability, and maladaptive cognitive processing. Unlike substance-related disorders, DA involves excessive engagement with rewarding digital stimuli (e.g., social media, online games, or mobile applications) without a clear physiological substrate, making its mechanisms primarily psychological and behavioral. Several theoretical models support this view, converging on the idea that digital overuse functions as a coping mechanism for managing negative emotions and environmental stressors.
The Cognitive Behavioral Model is one of the most widely adopted, emphasizing the role of automatic thoughts and dysfunctional beliefs in maintaining maladaptive behaviors (Beck, 1979). Cognitive behavioral therapy (CBT)–based interventions thus aim to correct these distorted cognitions, while also providing structured emotional regulation strategies and behavioral alternatives (Young, 1998).
Another relevant framework is the self-regulation theory (Carver & Scheier, 2001); maladaptive digital behaviors may result from impaired goal-directed control and an overreliance on short-term rewards. Adolescents, whose executive functioning and impulse control systems are still developing, are particularly susceptible to this imbalance. When emotional dysregulation is present, digital platforms may serve as a form of coping strategy based on avoidance. This aligns with Gross’s model of emotion regulation (Gross, 1998), which posits that individuals seek external behaviors to modulate internal states when they lack effective cognitive strategies. In this context, DA becomes a reinforcing cycle: emotional distress leads to digital engagement, which provides temporary relief but ultimately exacerbates dependence and avoidance patterns. Teaching adolescents to recognize and manage their emotional states is thus considered a key target in both prevention and treatment of DA (Lindenberg et al., 2020).
Incorporating these dimensions, the theoretical framework guiding this review posits that DA arises from an interaction between individual vulnerabilities (e.g., impulsivity, affective dysregulation), environmental reinforcements (e.g., accessibility, peer norms), and cognitive distortions. Effective interventions, therefore, must be multidimensional: they should target not only the behavior itself but also the underlying emotional and cognitive mechanisms that drive it. This perspective supports a structured overview of existing therapeutic and preventive programs, highlighting their contextual diversity and general approaches while pointing to the need for deeper analysis of how they target the core mechanisms of DA.
Materials and Methods
Search Strategy
This review followed the PRISMA 2020 guidelines for reporting systematic and narrative reviews (Page et al., 2021). The PRISMA 2020 full checklist is provided as a supplementary file. As this is a narrative review synthesizing empirical studies and not a meta-analysis or clinical trial, no PROSPERO or OSF registration was conducted.
A comprehensive literature search was executed using several databases including ScienceDirect, PsycInfo, PubMed, and Scopus. The search aimed to identify empirical studies on interventions targeting DA among adolescents. The search terms were constructed around four conceptual components: the type of digital use, the nature of the disorder, the population, and the type of intervention. Especially, the Boolean operators used were (digital OR internet OR smartphone OR social media) AND (addiction OR compulsive) AND (adolescent OR youth) AND (treat* OR prevent* OR combat*). Search strings were tailored to the syntax of each database.
In PubMed, this research was applied in the “title/abstract” fields using both controlled vocabulary (MeSH terms) and free-text keywords. In Scopus, the query was formulated to include title, abstract, and keyword fields using the “TITLE-ABS-KEY” operator, with access obtained via institutional academic account. In Web of Science, the search was conducted using the “Topic” field, which encompasses titles, abstracts, author keywords, and Keywords Plus. In PsycINFO, subject headings and abstract fields were utilized to retrieve records relevant to psychological interventions. Finally, in ScienceDirect, keyword combinations were searched across full texts and abstracts within the health and psychology domains.
All searches were limited to peer-reviewed journal articles published in English and available in open access. The time frame was restricted to publications from 2013 to 2023, corresponding to the period leading up to the literature search. Search results were exported to Zotero reference manager, and duplicates were identified automatically and removed manually using Zotero’s duplicate detection tool. Title and abstract screening were performed by two independent reviewers, with disagreements resolved through discussion.
Inclusion and Exclusion Criteria
Inclusion criteria encompassed studies that were (1) published between 2013 and 2023, (2) grounded in empirical evidence, (3) featured in peer-reviewed journals, (4) published in English, and (5) available as open-access resources. Conversely, studies were excluded if they (1) inadequately detailed the employed countermeasures, (2) failed to discuss the efficacy of the countermeasures, (3) pertained to participants outside the adolescent age bracket (12–18 years), (4) were conference abstracts, editorials, doctoral dissertations, reviews, theoretical papers, or case studies, and (5) revolved around gambling. Excluding gambling studies was due to the potential overlap between the terms “gaming” and “gambling” in the research literature. Additionally, the absence of a consensus on categorizing DA as a mental disorder, combined with the recent recognition of Gaming Disorder by the World Health Organization in the International Classification of Diseases, prompted the omission of Gambling Disorder from the search. This strategic decision aimed to prevent any distortion of the understanding of DA as a condition and the subsequent analysis of countermeasure efficacy.
Gray literature (e.g., reports, dissertations, non-peer-reviewed articles, and conference proceedings) was excluded to ensure the scientific rigor and reproducibility of the findings. Given the emerging nature of DA research, only empirical studies published in peer-reviewed journals were included, which meet the quality standards necessary to draw valid and generalizable conclusions.
Data Extraction
The database exploration took place on August 13, 2023. Data extraction was meticulously carried out from each selected study. The extracted information included:
- Country of study and study settings.
- Demographics of the study population (number of participants, age, gender).
- Specifics of DA behaviors.
- Diagnostic instruments used.
- Types of interventions implemented.
- Study designs and methodologies.
- Duration of interventions and follow-up periods.
- Outcomes measured and results obtained.
- Pre- and post-intervention means and baseline standard deviations for the relevant outcome measures, to allow effect size calculation.
This structured approach to data extraction ensured a comprehensive understanding of the interventions and their outcomes, facilitating a thorough synthesis of the existing literature.
Given the narrative nature of this review and the heterogeneity of study designs, no formal risk of bias assessment (e.g., using RoB 2 or JBI tools) was conducted. Instead, methodological strengths and limitations were discussed qualitatively in the Results and Discussion sections.
Data Analysis
The analysis focused on comparing the efficacy of different interventions, the extent of parental involvement, and the sustainability of outcomes over time. Special attention was given to the methodologies employed in these studies to ascertain the robustness of the findings and the applicability of the results across different settings.
Effect sizes were calculated using standardized mean differences, with the baseline standard deviation used as the denominator for within-group comparisons (d = [M_follow-up − M_baseline] / SD_baseline). This approach was selected to enable direct comparison across studies with varying designs, including both controlled and uncontrolled trials. Using the baseline standard deviation provides a consistent reference point representing natural population variability prior to any intervention, avoiding confounding effects from treatment-induced variance changes that may occur at follow-up assessments.
Although some studies reported multiple follow-up timepoints (e.g., 1, 4, and 12 months), effect sizes were deliberately calculated for each follow-up separately, rather than only the longest one, in order to highlight temporal patterns and observe whether treatment effects increased or decreased over time. This allowed us to detect a consistent trend across studies showing that treatment benefits tend to strengthen and become more pronounced at the 12-month follow-up.
Effect sizes were interpreted according to Cohen’s conventions, where d = 0.2 represents a small effect, d = 0.5 a medium effect, and d = 0.8 or higher a large effect. To correct for small sample bias, Hedges’ g was computed by applying a correction factor to each Cohen’s d value. This standardized procedure ensures methodological consistency across the diverse designs and outcome measures included in this review.
Results
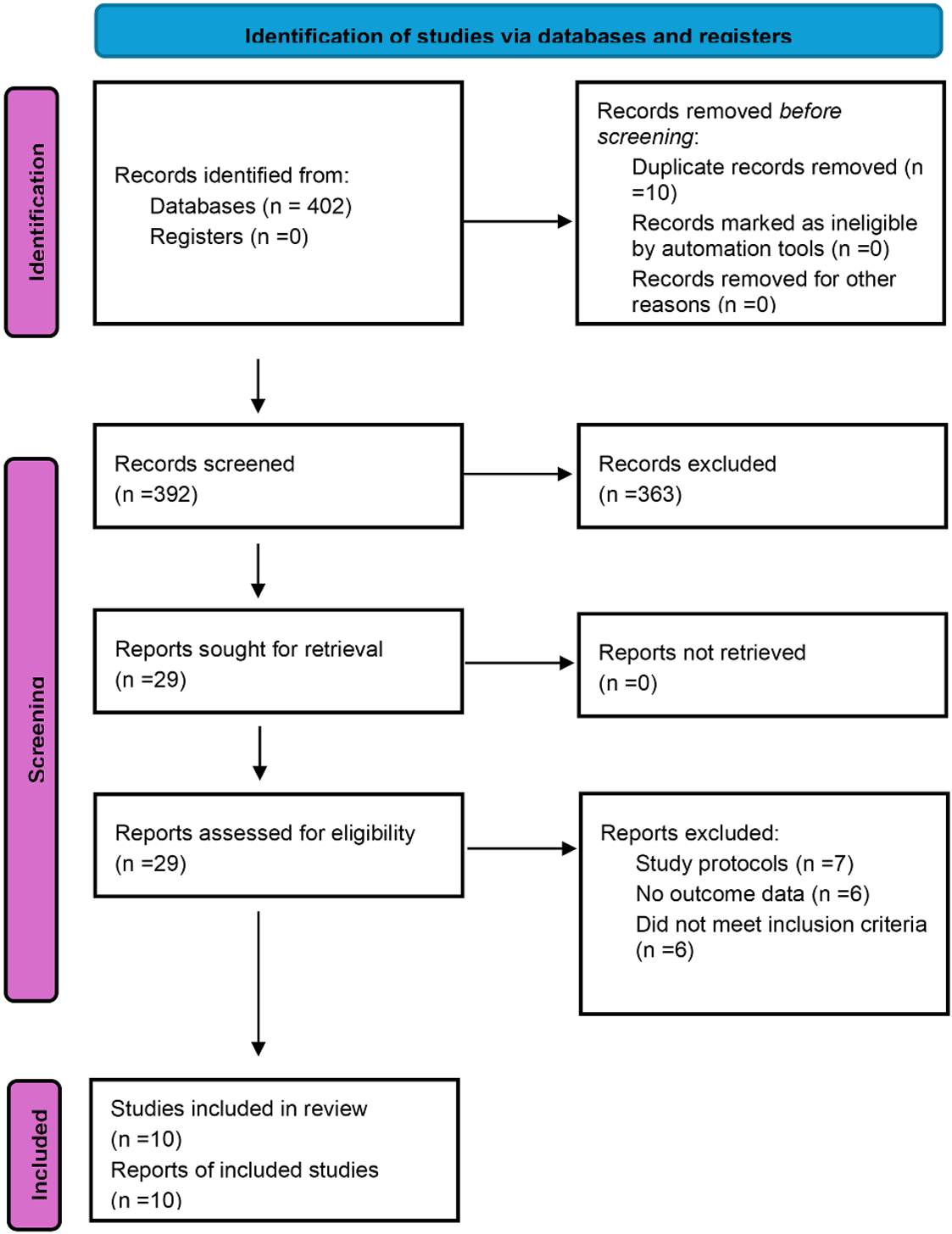
The systematic search and selection process yielded a total of 402 studies initially, which were then screened based on titles and abstracts, resulting in 29 papers that were further assessed for eligibility. After examining the method and results, 19 studies were excluded as they were either study protocols, did not report results, or presented any exclusive criteria discussed below. As a result, 10 studies were included in this review. The selection process is illustrated in Figure 1.
Selected Studies
The selected studies have a significant impact within the academic community. All included studies, regardless of when they were published, provide valuable insights that drive ongoing discussions and developments in understanding DA among adolescents (Table 1).
| Table 1. Citation impact of studies on digital addiction among adolescents | ||
| Author |
|
Title |
| Kor & Shoshani. |
|
Moderating the impact of covid 19 pandemic on children’s and adolescents’ substance use, digital media use and mental health: a randomized positive psychology addiction prevention program. |
| Lindenberg et al. |
|
Effectiveness of cognitive behavioral therapy-based in preventing disorder and unspecified internet use disorder in adolescents. |
| Bong et al. |
|
Effect of cognitive behavioral therapy-based music therapy in Korean adolescents with smartphone and internet addiction. |
| Szász-Janocha et al. |
|
Treatment outcomes of CBT based group intervention for adolescents with internet use disorder. |
| Nielsen et al. |
|
Multidimensional family therapy reduces problematic gaming in adolescents: A randomized controlled trial. |
| Choi et al. |
|
The Effect of Mind Subtraction Meditation Intervention on Smartphone Addiction and the Psychological Wellbeing among Adolescents. |
| Torres-Rodríguez et al. |
|
Treatment efficacy of a specialized psychotherapy program for internet gaming disorder. |
| Kim et al. |
|
A Preliminary Study on the Effectiveness of the Peer Relationship Enhancement Program in Adolescents at Risk for Internet and Smartphone Addiction. |
| González-Bueso et al. |
|
Internet Gaming Disorder in Adolescents: Personality, Psychopathology and Evaluation of a Psychological Intervention Combined With Parent Psychoeducation. |
| Lee et al. |
|
The effect of home-based daily journal writing in Korean adolescents with smartphone addiction. |
Although only 10 studies met the inclusion criteria, this was not a deliberate limit but the actual outcome of a rigorous selection process. Despite the small number, thematic saturation was reached, as the studies consistently highlighted CBT as the main intervention and emphasized the importance of parental involvement. This convergence suggests that the data were sufficient to identify meaningful trends in adolescent DA interventions.
Experimental Approaches and Intervention Effectiveness
Out of the 10 studies analyzed, seven employed an experimental trial approach to explore the effectiveness of various interventions (Bong et al., 2021; Choi et al., 2020; González-Bueso et al., 2018; Kim et al., 2018; Kor & Shoshani, 2023; Nielsen et al., 2021; Torres-Rodríguez et al., 2018). Within this subgroup, four studies tested different countermeasures across multiple participant groups to assess their impact (Bong et al., 2021; González-Bueso et al., 2018; Nielsen et al., 2021; Torres-Rodríguez et al., 2018), while three studies focused on monitoring changes over time within a single group by comparing initial and follow-up data (Lee et al., 2016; Lindenberg et al., 2022; Szász-Janocha et al., 2021). Additionally, three of these experimental studies included control groups without interventions (Choi et al., 2020; Kim et al., 2018; Kor & Shoshani, 2023), which were crucial for evaluating the effectiveness of the countermeasures.
Study Characteristics
Most of the research was conducted in South Korea, with four studies originating from this country, followed by Germany and Spain with two studies each, and Switzerland and Israel contributing one study each (Figure 2).
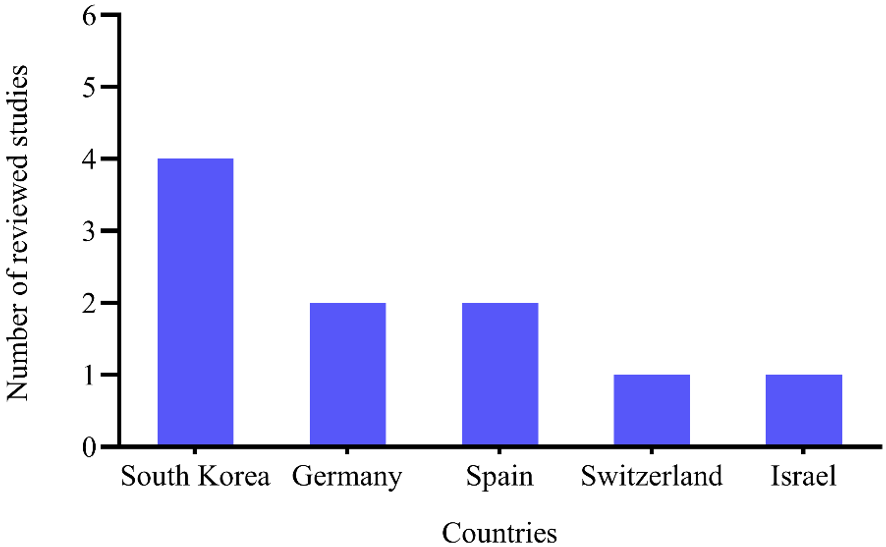
South Korea’s active involvement in researching the treatment of DA in adolescents is confirmed in many reviews (Cemiloglu et al., 2022; Karakose et al., 2022; Schneider et al., 2017). This can be attributed to the nation’s technological advancements and high rates of internet and smartphone usage that have created a fertile ground for studying the impact of digital devices on youth. This geographic distribution highlights the global concern regarding DA among adolescents but also points to a concentration of research activity in regions with high digital connectivity.
Screening Instruments and Diagnostic Criteria
The Korean Smartphone Addiction Proneness Scale was the most frequently utilized screening instrument, employed in four studies. Other notable instruments included the Compulsive Internet Use Scale and the German Video Game Dependency Scale. The use of multiple diagnostic tools reflects the complexity of diagnosing DA, which lacks uniform diagnostic criteria globally. Table 2 provides a detailed list of the screening instruments used across the reviewed studies.
| Table 2. Digital addiction screening instruments utilized by countermeasure studies | ||
| Digital addiction screening instrument | Studies |
|
| Compulsive Internet Use Scale CIUS (Meerkerk et al., 2010) | (Szász-Janocha et al., 2021) |
|
| German Video Game Dependency Scale CSAS (Rehbein et al., 2015) | (Lindenberg et al., 2022; Szász-Janocha et al., 2021) |
|
| Screen time scale (Mark & Janssen, 2008) | (Kor & Shoshani, 2023) |
|
| Petry’s IGD scale ( Petry & O’Brien, 2013 ) | (Nielsen et al., 2021) |
|
| DSM 5 IGD criteria (American Psychiatric Association, 2013) | (Lindenberg et al., 2022; Nielsen et al., 2021; Szász-Janocha et al., 2021; Torres-Rodríguez et al., 2018) |
|
| Abbreviated Self Completion Teen-Addiction Severity Index (ASC T-ASI) (Reckers-Droog et al., 2020 ) | (Nielsen et al., 2021) |
|
| Internet gaming disorder test IGD-20 Pontes, 2014) | (Torres-Rodríguez et al., 2018) |
|
| Motivation scale for smartphone regulation (Individual Counseling Manual for Smartphone Addiction. Seoul: Ministry of Gender Equality & Family, 2013) | (Lee et al., 2016) |
|
| Korean Smartphone Addiction Proneness Scale (Kim et al., 2014) | (Bong et al., 2021; Choi et al., 2020; Kim et al., 2018; Lee et al., 2016 |
|
| DQVMIA diagnostic questionnaires for video games, mobile phone or internet addiction ( Stinchfield, 2003) | (González-Bueso et al., 2018) |
|
| Young internet addiction scale YIAT Young, 1998) | (Bong et al., 2021) |
|
| Korean Internet Addiction Proneness Scale (Kim et al., 2008) | (Kim et al., 20018) |
|
Digital Addiction Types
Digital addiction types that have been examined in the studies are IGD, smartphone addiction, internet addiction, and digital media addiction. Figure 3 offers a cumulative view of the research conducted on DA, categorizing the total number of studies by addiction type.
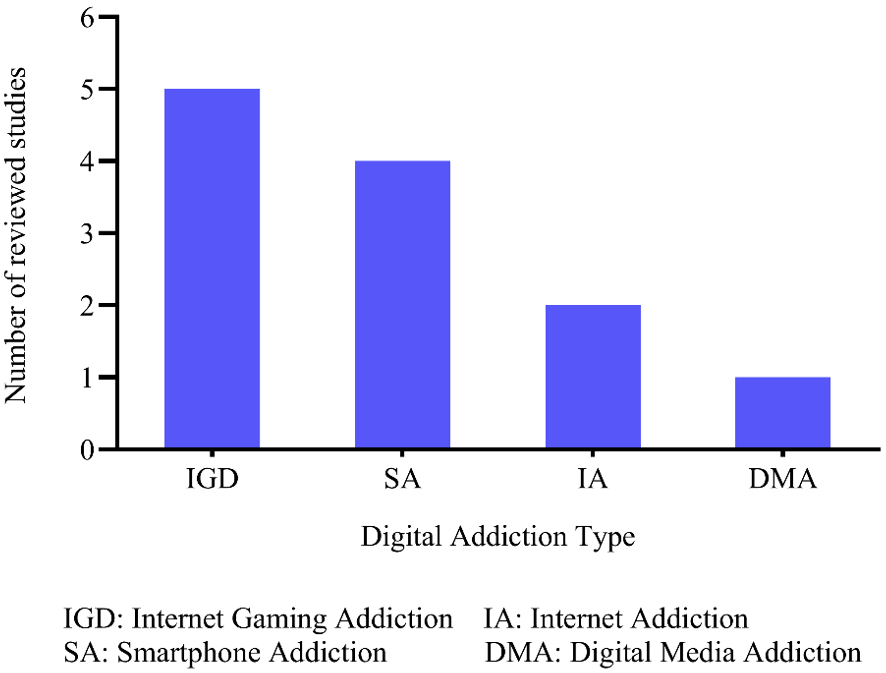
IGD is the most studied type of DA followed by smartphone addiction, indicating a significant scholarly focus on gaming behaviors, possibly due to its formal recognition in diagnostic criteria and the widespread prevalence of gaming. This emphasis on IGD and smartphone addiction suggests that these forms of digital behavior are considered to have substantial impacts on adolescents, warranting extensive research to develop targeted intervention strategies.
Considering research on DA trends, Figure 4 maps the evolution of DA types considered in the studies selected.
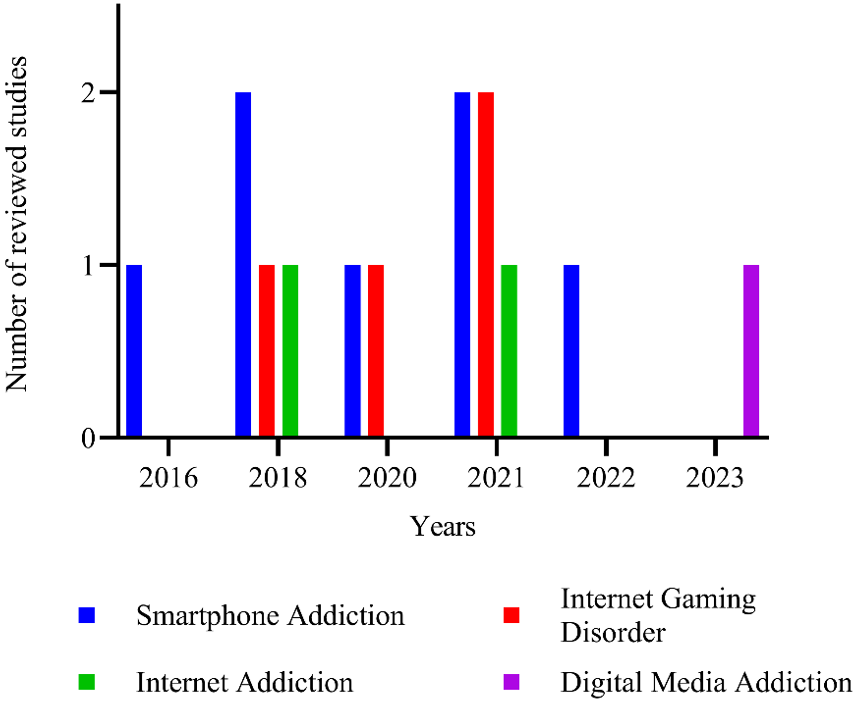
This temporal perspective is important to understand the evolution of research interests and responsiveness of the academic community to emerging trends. The graphic shows a peak in studies on smartphone addiction in 2018 as a response to the proliferation of these devices. Meanwhile, the recent rise in digital media addiction studies indicates an adaptive focus on new and evolving forms of DA.
Intervention Effectiveness
In the domain of intervention strategies, different approaches and methodologies were applied across different studies. The systematic comparison highlights the diversity of experimental interventions targeting DA by examining key parameters such as study design, participant characteristics, age range, extent of parental involvement, the nature of the intervention, number of sessions, as well as the presence and duration of follow-up periods (Table 3).
| Note: N, Participants; IGD, Internet Gaming Disorder; CBT, Cognitive Behavioral Therapy; MT, Musical Therapy; MDFT, Multi-Dimensional Family Therapy; RCT, Randomized Controlled Trial. | |||||||
| Table 3. Summary of study characteristics and intervention details | |||||||
| Reference | Design | N | Age | Parent participation | Intervention type | Sessions | Follow up |
| (Kor & Shoshani, 2023) | RCT | 1670 | 10 to 16 | no | Positive psychology addiction prevention PPAP | 30 units lasting two hours each | 3 years longitudinal repeated measures |
| (Lindenberg et al., 2022) | RCT | 422 | 12 to 18 | no | CBT based group program protect+ | 4 weekly sessions | After 1, 4 and 12 months |
| (Bong et al., 2021) |
Two-arm, non-RCT |
155 | 10 to 16 | no | CBT and CBT with MT | 8 sessions of 75 min | no |
| (Szász-Janocha et al., 2021) | Single-arm longitudinal study | 54 | 9 to 19 | no | CBT based group program protect+ | 4 weekly sessions | After 4 and 12 months |
| (Nielsen et al., 2021) | RCT | 42 | 12 to 19 | Family therapy | MDFT Vs Family therapy as usual | 6 months | 12 months |
| (Choi et al., 2020) |
Two-arm, non-RCT |
49 | 16 | no | Meditation intervention | 20 min per session in the morning 2 times a week for 12 weeks | 4 weeks after completion |
| (Torres-Rodríguez et al., 2018) |
Two-arm Non-RCT |
31 | 12 to 18 | Family intervention | PIPATIC program is a specialized program for adolescent’s IGD (CBT approach) | 22 sessions of 45 min weekly for 6 months | After 3 months |
| (Kim et al., 2018) | pre-post quasi-experimental design | 33 | 14 to 15 | no | Peer Relationship enhancement program, CBT program | 8 sessions of 50 min once a week | no |
| (González-Bueso et al., 2018) | Quasi experimental two-arm study | 30 | 12 to 21 | Psychoeducational group for parents | CBT or CBT plus psychoeducation for parents |
12 sessions of 45 min: 4 sessions weekly, 4 sessions biweekly and 4 sessions monthly |
no |
| (Lee et al., 2016) | Quasi experimental pre-post study | 335 | 12 to 19 | Discuss the issue with parents | Home based daily journal of smartphone use based on CBT | 2 weeks | no |
A significant number of the studies reviewed utilized CBT-based interventions (Bong et al., 2021; González-Bueso et al., 2018; Kim et al., 2018; Lee et al., 2016; Lindenberg et al., 2022; Szász-Janocha et al., 2021), with seven out of ten studies incorporating this approach. Additionally, various other interventions are used: peer relationship enhancement (Kim et al., 2018), meditation program (Choi et al., 2020), Multi-Dimensional Family Therapy (MDFT) (Nielsen et al., 2021), and Positive Psychology Addiction Prevention (PPAP) (Kor & Shoshani, 2023).
The interventions varied significantly in terms of duration, ranging from four sessions over a month (Lindenberg et al., 2022; Szász-Janocha et al., 2021) to programs extending up to six months (Nielsen et al., 2021). Parental involvement was reported in 40% of the studies (González-Bueso et al., 2018; Lee et al., 2016; Nielsen et al., 2021; Torres-Rodríguez et al., 2018), indicating a recognition of the role families play in the treatment process.
Long-term follow-up was inconsistent across studies, with 60% conducting follow-ups to assess the sustainability of the results (Choi et al., 2020; Kor & Shoshani, 2023; Lindenberg et al., 2022; Nielsen et al., 2021; Szász-Janocha et al., 2021; Torres-Rodríguez et al., 2018). Notably, studies without follow-up evaluations highlighted a significant gap in understanding the long-term efficacy of interventions.
Effect Sizes of Intervention Studies on Digital Addiction
Across the 10 studies, means, standard deviations, and sample sizes were extracted for each intervention group at all available time points (baseline and follow-up). For each comparison (e.g., baseline → 6 months, baseline → 12 months), Cohen’s d was first computed using the pooled within-group standard deviation. To correct for small sample bias and ensure comparability across studies, each d value was multiplied by Hedges’ correction factor (J = 1 − 3 / (4N − 9)), where N is the total sample size, yielding Hedges’ g. These g values, calculated separately for each group and outcome, form the basis for the cross-study effect size synthesis presented in Table 4.
| Note: n.d., No Data; STS, Screen Time Scale; CSAS, German Video Game Dependency Scale; YIAT, Young Internet Addiction Scale; CIUS, Compulsive Internet Use Scale; German Video Game Dependency Scale-Self Report; CSAS-PR, German Video Game Dependency Scale-Parental Report; MDFT, Multidimensional Family Therapy; FTAU, Family Therapy As Usual; IGD, Internet Gaming Disorder; IGD-20, Internet Gaming Disorder Test; CBT, Cognitive Behavioral Therapy; KIAPS, Korean Internet Addiction Proneness Scale; KSAPS, Korean Smartphone Addiction Proneness Scale; DQVMIA, diagnostic questionnaires for video games, mobile phone or internet addiction. | |||||||
| Table 4. Summary of study characteristics and intervention details | |||||||
| Study | Scale | T1 | T2 | T3 | |||
| (Kor & Shoshani, 2023) | STS | Baseline |
Post intervention Cohen’s d = 0.002 Hedges’ g = 0.002 |
After 12 months Cohen’s d = 0.05 Hedges’ g = 0.048 |
|||
| (Lindenberg et al., 2022) |
CSAS (inter-group effect size) |
After 1 month Cohen’s d = 010 Hedges g = 0.095 |
After 4 months Cohen’s d = 0.22 Hedges g = 0.22 |
After 12 months Cohen’s d = 0.67 Hedges g = 0.665 |
|||
| (Bong et al., 2021 | CBT group | YIAT |
Post intervention Cohen’s d = 0.59 Hedges g = 0.59 |
n.d. | n.d. | ||
| SAPS |
Cohen’s d = 0.73 Hedges g = 0.73 |
n.d. | n.d. | ||||
| CBT+MT group | YIAT |
Cohen’s d = 1.06 Hedges g = 1.05 |
n.d. | n.d. | |||
| SAPS |
Cohen’s d = 0.73 Hedges g = 0.72 |
n.d. | n.d. | ||||
| (Szász-Janocha et al., 2021) | CIUS |
Post intervention Cohen’s d = 0.059 Hedges g = 0.059 |
After 4 months Cohen’s d = 0.219 Hedges g = 0.216 |
After 12 months Cohen’s d = 1.003 Hedges g = 0.989 |
|||
| CSAS-SR |
Cohen’s d = 0.049 Hedges g = 0.048 |
Cohen’s d = 0.230 Hedges g = 0.227 |
Cohen’s d = 0.741 Hedges g = 0.731 |
||||
| CSAS-PR |
Cohen’s d = 0.854 Hedges g = 0.843 |
Cohen’s d = 0.645 Hedges g = 0.636 |
Cohen’s d= 0.960 Hedges g = 0.946 |
||||
| (Nielsen et al., 2021) | Petry’s IGD scale | MDFT intervention | n.d. |
After 6 months n.d. |
After 12 months n.d. |
||
| FTAU intervention | n.d. | n.d. | n.d. | ||||
| (Choi et al., 2020) | KSAPS |
Post intervention Cohen’s d = 0.59 Hedges g = 0.57 |
After 1 month Cohen’s d = 1.04 Hedges g = 1.01 |
n.d. | |||
| Torres-Rodríguez et al., 2018) | IGD-20 | PIPATIC intervention |
Post intervention n.d. |
After 3 months n.d. |
n.d. | ||
| CBT intervention | n.d. | n.d. | n.d. | ||||
| (Kim et al., 2018) | KIAPS |
Post intervention Cohen’s d = 1.16 Hedges g = 1.13 |
n.d. | n.d. | |||
| KSAPS |
Post intervention Cohen’s d = 0.94 Hedges g = 0.92 |
n.d. | n.d. | ||||
| (González-Bueso et al., 2018) | DQVMIA |
Post intervention Cohen’s d = 1.17 Hedges g = 1.14 |
n.d. | n.d. | |||
| (Lee et al., 2016) | KSAPS |
Post intervention Cohen’s d = 0.74 Hedges g = 0.73 |
n.d. | n.d. | |||
Kor & Shoshani (2023) evaluated the effect of a school-based positive psychology intervention on adolescents’ screen-related behaviors using the Screen Time Scale. This scale assessed daily recreational use across television/internet, social media, and gaming, summed into a total score. For the intervention group, screen time remained stable from baseline (T1) to post-intervention (T2), with a calculated effect size of Hedges’ g = 0.002, indicating no meaningful change. At 12-month follow-up (T3), the change was still minimal (g = 0.048), consistent with the author-reported within-group effect of Cohen’s d = 0.05 in Table 3. In contrast, the control group showed a moderate increase in screen time both post-intervention (g = 0.273) and at follow-up (g = 0.337). Although the authors mention a medium effect size (d = 0.60) in the text, this likely refers to a between-group intervention effect rather than a within-group change. These findings suggest that the intervention was effective in stabilizing screen time over time, while the control group experienced notable increases.
To quantify the effectiveness of the PROTECT intervention reported by Lindenberg et al. (2022), symptom severity scores of Internet Use Disorder were examined using the CSAS scale at four time points: baseline (T0), 1-month (T1), 4-month (T2), and 12-month follow-up (T3). The authors reported a Cohen’s d of 0.67 for the PROTECT group from baseline to 12 months, reflecting a moderate to large effect size. To complement this, Cohen’s d and Hedges’ g were calculated at earlier follow-up points using the means and standard deviations provided in Supplementary Table 2. For the PROTECT group, the effect size at 1 month was small (g = 0.095), while a modest reduction in symptom severity was observed at 4 months (g = 0.22). These estimates were derived using the pooled standard deviation between baseline and each respective follow-up. Importantly, all effect size calculations were based on the same instrument (CSAS) administered consistently across all time points, ensuring the methodological validity of within-group comparisons.
In the study by Bong et al. (2021), the authors did not report any effect size indices for within-group changes. Therefore, Cohen’s d and Hedges’ g were calculated using pre- and post-intervention means, with baseline standard deviations as denominators to ensure consistency across studies. For the Young Internet Addiction Test (YIAT), the CBT + MT group showed a large within-group effect (Hedges’ g = 1.05), whereas the CBT-only group demonstrated a moderate effect (g = 0.59), suggesting a stronger impact when music therapy was added to cognitive-behavioral treatment. In contrast, for the Smartphone Addiction Proneness Scale (SAPS), both groups showed similar moderate-to-large effect sizes (g = 0.72 for CBT + MT and g = 0.73 for CBT), indicating that both interventions were comparably effective in reducing smartphone-related addictive behaviors. Notably, no follow-up assessments were conducted beyond the 8-week intervention period, limiting conclusions regarding the durability of treatment effects.
The original article by Szász-Janocha et al. (2021) reported within-group effect sizes (Cohen’s d) only for the change between baseline and 12-month follow-up. The recalculated values closely match the authors’ reported d values across all three primary outcome measures (CIUS, CSAS-SR, CSAS-PR), suggesting that a similar computation method was used. Minor differences (e.g., d = 0.960 vs. 0.961) are likely due to rounding. However, unlike the original study, Hedges’ g was also calculated to correct for small sample bias, and effect sizes at additional time points (post-intervention and 4-month follow-up). This offers a more detailed picture of the intervention’s progression over time and ensures consistency across all studies included in this review.
The study by Nielsen et al. (2021) assessed the severity of IGD using the DSM-5 criteria with Petry’s 9-item dichotomous scale. While the article reports pre–post reductions in IGD symptom count for both the MDFT and Family therapy as usual (FTAU) groups, group-specific means and standard deviations were only partially available. Although intergroup effect sizes were reported by the authors (Cohen’s d = 1.23 at 6 months and d = 0.93 at 12 months), the lack of sufficient data (e.g., SDs at follow-up per group, or exact within-group means) prevented us from recalculating intra-group effect sizes using the standardized formula based on baseline SDs. As a result, this study was excluded from the pooled within-group meta-analytic comparison to ensure methodological consistency across studies. However, its intergroup effect sizes remain informative and indicate a moderate-to-large advantage for MDFT over FTAU in reducing IGD symptoms over time.
In the study by Choi et al. (2020), the authors did not report effect sizes; therefore, effect sizes were calculated based on the total score of the Korean Smartphone Addiction Proneness Scale (KSAPS) using the standardized mean difference, with the baseline standard deviation as the denominator. For the experimental group, the KSAPS total score decreased from 33.88 (SD = 7.19) at baseline to 29.63 post-intervention and 26.38 at one-month follow-up. This corresponds to a medium within-group effect immediately post-intervention (g = 0.57), and a large effect at follow-up (g = 1.01), suggesting that the impact of the mind subtraction meditation program not only persisted but continued to strengthen in the weeks following the intervention.
For the study by Torres-Rodríguez et al. (2018), standardized effect sizes could not be calculated due to the lack of means and standard deviations at follow-up points; only median scores and a baseline standard deviation were reported. Attempts to compute Hedges’ g from these data yielded implausibly inflated values, likely due to the combination of very low baseline variance and large observed reductions. Nevertheless, the study reported a substantial drop in IGD symptoms: in the PIPATIC group, the IGD-20 score decreased from a baseline median of 79.75 to 32.19 post-treatment and 30.69 at 3-month follow-up. In the CBT control group, scores decreased from 76.13 to 51.93 post-treatment, then slightly increased to 56.40 at follow-up. These results suggest clinically meaningful improvement, especially in the integrative PIPATIC condition, despite the absence of standardized effect size estimates. While these changes appear clinically meaningful, the lack of valid effect size estimates led us to exclude this study from the quantitative comparison table.
Kim et al. (2018) conducted a pre-post quasi-experimental study to evaluate the Peer Relationship Enhancement Program among adolescents at risk for Internet and smartphone addiction. Using the Korean Internet Addiction Proneness Scale (KIAPS) and Korean Smartphone Addiction Proneness Scale (KSAPS), they reported significant reductions in both scores after the 8-week intervention. Although the authors did not report effect sizes, within-group standardized mean differences were calculated using baseline standard deviations. For KIAPS, the effect size was d = 1.16 and Hedges’ g = 1.13, indicating a large effect. For KSAPS, d = 0.94 and g = 0.92, also reflecting a large effect. These findings support the short-term efficacy of the intervention in reducing self-reported DA symptoms.
González-Bueso et al. (2018) did not report standardized effect sizes such as Cohen’s d or Hedges’ g. Following the method, within-group effect sizes for the DQVMIA total score were calculated using the baseline standard deviation as the denominator. The mean score decreased from 6.20 at baseline to 4.37 post-intervention (SD = 1.56), yielding an effect size of Cohen’s d = 1.17 and Hedges’ g = 1.14. These values reflect a very large improvement in IGD symptomatology following the CBT intervention. Using the baseline SD ensures comparability across studies by avoiding bias from post-treatment variance reduction.
Lee et al. (2016) evaluated the effect of a two-week home-based daily journal (HDJ-S) on smartphone addiction among Korean adolescents identified as high risk, using the Korean Smartphone Addiction Proneness Scale (KSAPS). While the authors reported a significant pre-post reduction in KSAPS scores (t = 5.87, p < .001), they did not report standardized effect sizes. Following the method, within-group effect sizes were calculated using the baseline standard deviation: Cohen’s d = 0.76 and Hedges’ g = 0.74, both indicating a moderate treatment effect. These results suggest that the HDJ-S may be an effective short-term strategy to reduce problematic smartphone use in high-risk adolescents, although the absence of a control group limits causal interpretations.
Areas for Future Research
The increasing availability of self-help software applications aimed at helping individuals manage their digital device usage marks a significant trend (Haug et al., 2020; Lin et al., 2017). The analysis of selected studies shows the absence of software-mediated therapies suggesting a potential area for future exploration. Such interventions could offer scalable solutions to reach a broader audience and provide more flexible treatment options for DA.
Discussion
The findings from this narrative review highlight significant insights into the prevention and therapy interventions for DA among adolescents. This discussion contextualizes these findings within the broader landscape of current research, challenges faced, and potential future directions.
Screening Instruments and Diagnostic Complexity in Digital Addiction
Exploring interventions for a condition that lacks clear definition is a significant challenge. For instance, while Gaming Disorder is recognized as a diagnosable clinical disorder under both the American Psychiatric Association and the World Health Organization criteria, other forms of DA, such as internet or social media use, do not currently meet the criteria for diagnosis under these systems. This discrepancy raises important questions about the appropriate terminology to use when discussing interventions and changes in these behaviors.
Despite these challenges, there is a growing trend to treat all forms of DA as behaviors associated with harm that individuals might want to change. The evolution of digital media over the past decade has influenced the development of screening instruments, which have traditionally focused more on the psychological impacts and related harmful consequences than on the digital medium itself (Cemiloglu et al., 2022). The evolution of internet addiction screening instruments has been influenced by the emergence of new technologies and media. Chóliz proposed three screening tools for different technological addictions, including internet and social networks (Chóliz et al., 2017). Lortie highlighted the need for refinement in the design of internet addiction assessment tools, particularly in the representation of the social dimension (Lortie & Guitton, 2013). Laconi et al. (2014) emphasized the importance of further validation work for existing scales (Laconi et al., 2014). These studies collectively underscore the ongoing evolution and refinement of internet addiction screening instruments in response to the changing landscape of internet media and connected devices.
Furthermore, most of the studies combined multiple diagnostic tools due to the lack of uniform diagnostic criteria. Some of the reviewed studies assess the effectiveness of interventions based on the reduction of time spent on digital devices post-intervention. While this measure is critical in evaluating the outcomes of countermeasures, it may oversimplify the complex nature of DA. Time spent on devices alone does not necessarily reflect problematic usage, as the use might be intentional and important to the individual. Moreover, focusing solely on reduced screen time addresses only one symptom of DA and overlooks other dimensions of the condition. It is possible for individuals to suffer from DA without exhibiting excessive usage patterns, highlighting the need for a more nuanced approach to diagnosing and treating this modern malaise.
Comparison with Existing Literature
The reliance on CBT aligns with existing literature that recognizes CBT as one of the most effective approaches for treating various forms of addiction, including DA. The predominance of CBT-based interventions in research may be attributed to its well-established theoretical framework and extensive empirical validation in treating behavioral addictions (Han et al., 2020). In contrast, alternative interventions such as family therapy, mindfulness-based programs, or positive psychology interventions are relatively newer and may lack standardized protocols, making them harder to assess through controlled trials. Furthermore, many intervention studies focus on short-term efficacy, whereas approaches like mindfulness and family therapy often require long-term engagement, which may pose methodological challenges for researchers (Shin et al., 2021). Future studies should explore the potential of these alternative interventions, particularly in culturally diverse contexts where family dynamics play a significant role in adolescent digital behavior.
Within the context of DA, CBT was used to increase self-awareness on addictive usage by highlighting internal and external triggers that challenge their impulse control and by highlighting feelings, psychological needs, and cognitive distortions behind excessive use (Han et al., 2020). For instance, the “all or nothing thinking” where individuals may see their digital interactions as either completely rewarding or a total waste, with no middle ground; they might believe that if they’re not always connected, they are completely out of the loop or socially isolated. CBT aims to challenge these distortions by examining evidence against extreme beliefs and developing more balanced, realistic thoughts. Clients engage in behavioral experiments to test these new perspectives, helping them realize that not being constantly online does not result in extreme social isolation. This process is supported by skill-building activities that enhance offline interactions and manage online time, fostering healthier digital habits and reducing dependency on constant connectivity (Lindenberg et al., 2020).
It is noteworthy that most of the studies included in this review originate from South Korea, Germany, and Spain. This reflects the current distribution of research on intervention strategies for adolescent DA, rather than a limitation of the review itself, as the selection process was strictly based on predefined inclusion and exclusion criteria. While research on DA exists globally, studies specifically evaluating remediation methods for adolescents appear to be concentrated in a few countries, particularly those with structured national programs addressing problematic digital use (Chun et al., 2017). This suggests that the gap is not necessarily in the study of DA itself, but in the development and empirical evaluation of adolescent-targeted intervention programs across diverse cultural contexts. Future research should aim to expand the examination of such interventions to a wider range of countries to improve the generalizability of findings.
The role of parental involvement in the treatment of adolescent DA cannot be overstated. The review found that interventions incorporating a family approach tended to report better outcomes, echoing the findings of Shin (2021), who emphasized the critical role families play in the management and recovery from DA (Shin et al., 2021) . This underscores the necessity for intervention programs to not only target the adolescents but also engage their families to maximize the effectiveness of the treatments.
Intervention Effectiveness Based on Effect Sizes
The reviewed intervention studies targeting DA in adolescents demonstrate considerable variability in effect sizes, reflecting differences in intervention types, study designs, measurement tools, and follow-up durations. Among the most effective programs were those combining multiple therapeutic components. For instance, Bong et al. (2021) reported large effects for the CBT + MT group (g = 1.05 on YIAT), compared to a moderate effect for CBT alone (g = 0.59), indicating the added value of music therapy. Similarly, Kim et al. (2018) and González-Bueso et al. (2018) both yielded large within-group effects (g ≈ 1.1), suggesting strong efficacy of their respective CBT-based interventions.
In contrast, Kor & Shoshani (2023) showed minimal change over time (g = 0.002–0.048), likely due to the universal prevention nature of the intervention and low initial symptom severity. Intermediate results were observed in studies like Lee et al. (2016) (g = 0.74) and Choi et al. (2020) (g = 0.57–1.01), reflecting effective, short-term reductions in smartphone addiction.
Longitudinally, Lindenberg et al. (2022) also showed a trend of progressive improvement, with Hedges’ g rising from 0.095 at 1-month follow-up to 0.22 at 4 months and reaching 0.665 at 12 months, indicating a moderate to large effect over time. Similarly, Szász-Janocha et al. (2021) provided follow-up data at three time points (post-intervention, 4 months, 12 months), revealing a steady increase in effect sizes as well (CIUS: g = 0.06 → 0.22 → 0.99), suggesting long-term consolidation of treatment gains.
However, two studies (Nielsen et al., 2021; Torres-Rodríguez et al., 2018) were excluded from quantitative comparison due to insufficient or incompatible data (missing SDs or median-only reporting), although descriptive results suggest clinical improvement.
Overall, the largest within-group effects were consistently observed in targeted or clinical interventions employing CBT (alone or in combination), while universal school-based programs tended to show smaller effects. The correction using Hedges’ g ensured consistency across studies, particularly for those with small sample sizes. These findings highlight the need for long-term follow-up and standardized reporting practices to enhance comparability and evidence synthesis in DA interventions.
Gaps and Limitations
An important limitation when comparing effect sizes across studies is the variability in follow-up duration. Some of the strongest treatment effects were only observed at the 12-month follow-up, suggesting that therapeutic benefits often emerge progressively over time. In contrast, several interventions (e.g., Kor & Shoshani, Choi et al., Lee et al.) conducted outcome assessments at much shorter time frames (4 to 6 weeks or 3 months), potentially underestimating the full impact of the intervention. This discrepancy makes direct comparison challenging, as studies with limited follow-up may report lower g values not due to lower efficacy, but simply due to insufficient time for behavior change to consolidate. Future research should prioritize longitudinal assessment designs to ensure fair and informative comparison across intervention types.
Furthermore, the absence of software-mediated therapies in the reviewed studies suggests a missed opportunity in adolescents’ treatment and prevention of DA, as these could potentially provide accessible, cost-effective, and wide-reaching interventions. Although various studies have explored the use of mobile applications and digital interventions for addressing DA, none met the inclusion criteria of this review, likely due to the focus on adolescent-specific interventions. This suggests that while such solutions may be available, their application in adolescent populations remains underexplored or underreported in empirical research. The integration of software-based approaches with traditional interventions could offer promising avenues for enhancing accessibility and adherence among adolescents, warranting further investigation in future studies.
Moreover, the use of self-reported data inherently carries several weaknesses that compromise the reliability and validity of the findings. For example, self-reported responses can be influenced by social desirability bias, where participants may underreport behaviors perceived as undesirable, or by memory recall bias, which affects the accuracy of reported data. According to Araujo et al., 2017 there is a considerable discrepancy between self-reported internet use and actual usage tracked via digital tools, noting that individuals with higher levels of internet use tended to significantly underreport their usage. These factors underscore the need for incorporating more objective measures alongside self-reports to ensure a more comprehensive understanding of DA and the efficacy of its interventions. One way to mitigate these limitations is to integrate passive data collection methods, such as smartphone usage tracking applications and real-time behavioral monitoring, which can provide more accurate and objective measurements of digital consumption patterns (Ellis et al., 2019). Additionally, combining self-reports with parental or teacher assessments could enhance reliability, particularly in adolescent populations where self-perception biases may influence responses. Future studies should prioritize mixed-method approaches that blend subjective self-reports with objective tracking tools to improve the accuracy of DA assessments.
Implications for Future Research
The current review has identified several areas ripe for further investigation. Future research should explore the development and effectiveness of software-mediated interventions, which could include apps or web-based programs designed to manage DA. Additionally, more rigorous longitudinal studies are needed to assess the long-term effectiveness of these interventions and the role of emerging technologies in both exacerbating and treating DA.
Theoretical and Practical Contributions
This review contributes to the theoretical understanding of DA by synthesizing findings from a decade of research, offering a clearer picture of effective strategies and highlighting the essential components of successful interventions. Practically, the findings can assist clinicians and policymakers in designing and implementing more effective strategies for combating DA, with an emphasis on family involvement and the potential for digital solutions. In educational settings, schools could integrate structured digital literacy programs and responsible technology use training into their curricula, focusing on self-regulation strategies for adolescents. Additionally, school counselors and educators should be equipped with screening tools to identify at-risk students early and provide targeted interventions. From a public health perspective, policymakers could develop national guidelines for healthy digital consumption, incorporating evidence-based prevention and intervention programs like those implemented for substance use prevention. Governments and NGOs could also collaborate to fund research on scalable, software-mediated interventions that can be widely distributed to adolescents and their families. Future work should explore how multi-sector collaboration can bridge the gap between research findings and policy implementation.
Conclusion
This narrative review has provided a comprehensive examination of the existing preventive and therapeutic interventions for DA among adolescents from 2013 to 2023. Through a meticulous review of peer-reviewed literature, this study has highlighted the effectiveness of various intervention strategies, particularly those based on CBT, and identified significant gaps in current research practices.
Major Findings
The findings of this review indicate that CBT-centric methods are both common and successful in addressing DA in adolescents. Parental participation has emerged as an essential element, significantly boosting intervention outcomes. A critical shortfall identified is the lack of sustained follow-ups in research, which are crucial to evaluating the long-term impact of treatments. Furthermore, an evident gap is the current absence of interventions supported by software, suggesting an avenue for future research and development.
Theoretical and Practical Implications
Theoretically, this review contributes to the understanding of DA by framing it within the context of adolescent-specific needs and the effectiveness of tailored interventions. Practically, the findings can assist clinicians and policymakers in designing and implementing more effective strategies for combating DA, with an emphasis on family involvement and the potential for digital solutions.
Recommendations for Future Research
Given the gaps identified, future research should focus on:
- Conducting long-term studies to evaluate the durability of the interventions’ effects.
- Investigating the role of emerging digital technologies in both exacerbating and alleviating DA.
- Future studies should also adopt an interdisciplinary approach, integrating insights from psychology, neuroscience, education, and technology studies to develop more holistic intervention frameworks. Collaboration between behavioral scientists, software developers, and policymakers could lead to the creation of adaptive intervention programs tailored to adolescent needs. Additionally, exploring the neurobiological mechanisms underlying DA could provide valuable insights into personalized treatment strategies. Such interdisciplinary efforts will be crucial in advancing the field and ensuring that interventions are both evidence-based and scalable across diverse populations.
As digital technologies continue to evolve and integrate deeper into daily life, understanding and addressing DA in adolescents is more crucial than ever. This review not only sheds light on effective intervention strategies but also paves the way for innovative approaches to enhance the resilience of young individuals against the challenges posed by DA.
Data availability statement
Data sharing is not applicable to this article as no new datasets were generated or analyzed during this study.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (5th ed). American Psychiatric Association.
- Araujo, T., Wonneberger, A., Neijens, P., & de Vreese, C. (2017). How much time do you spend online? Understanding and improving the accuracy of self-reported measures of Internet Use. Communication Methods and Measures, 11(3), 173-190. https://doi.org/10.1080/19312458.2017.1317337
- Bağatarhan, T., & Siyez, D. M. (2017). The effectiveness of a Cognitive-Behavioral prevention program for internet addiction. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 40(4), 767-792. https://doi.org/10.1007/s10942-021-00439-7
- Beck, A. T. (1979). Cognitive therapy and the emotional disorders. Penguin.
- Bong, S. H., Won, G. H., & Choi, T. Y. (2021). Effects of Cognitive-Behavioral Therapy based Music Therapy in Korean adolescents with smartphone and internet addiction. Psychiatry Investigation, 18(2), 110-117. https://doi.org/10.30773/pi.2020.0155
- Brand, M., Rumpf, H-Jü., Demetrovics, Z., Muller, A., Stark, R., King, D. L., Goudriaan, A. E., Mann, K., Trotzke, P., Fineberg, N. A., Chamberlain, S. R., Kraus, S. W., Wegmann, E., Billieux, J., & Potenza, M. N. (2020). Which conditions should be considered as disorders in the International Classification of Diseases (ICD-11) designation of “other specified disorders due to addictive behaviors”?. Journal of Behavioral Addictions, 11(2), 150-159. https://doi.org/10.1556/2006.2020.00035
- Carver, C. S., & Scheier, M. F. (2001). On the self-regulation of behavior. Cambridge University Press.
- Cemiloglu, D., Almourad, M. B., McAlaney, J., & Ali, R. (2022). Combatting digital addiction: Current approaches and future directions. Technology in Society, 68, 101832. https://doi.org/10.1016/j.techsoc.2021.101832
- Choi, E.-H., Chun, M. Y., Lee, I., Yoo, Y.-G., & Kim, M.-J. (2020). The effect of mind subtraction meditation intervention on smartphone addiction and the psychological wellbeing among adolescents. International Journal of Environmental Research and Public Health, 17(9), 3263. https://doi.org/10.3390/ijerph17093263
- Chóliz, M., Echeburúa, E., & Ferre, F. (2017). Screening tools for technological addictions: A proposal for the strategy of mental health. International Journal of Mental Health and Addiction, 15(2), 423-433. https://doi.org/10.1007/s11469-017-9743-1
- Chun, J., Shim, H., & Kim, S. (2017). A meta-analysis of treatment interventions for internet addiction among Korean adolescents. Cyberpsychology, Behavior and Social Networking, 20(4), 225-231. https://doi.org/10.1089/cyber.2016.0188
- Department of Education, Seoul National University. (2013). Individual counseling manual for smartphone addiction. Seoul: Ministry of Gender Equality & Family.
- Ellis, D. A., Davidson, B. I., Shaw, H., & Geyer, K. (2019). Do smartphone usage scales predict behavior?. International Journal of Human-Computer Studies, 130, 86-92. https://doi.org/10.1016/j.ijhcs.2019.05.004
- González-Bueso, V., Santamaría, J. J., Fernández, D., Merino, L., Montero, E., Jiménez-Murcia, S., Del Pino-Gutiérrez, A., & Ribas, J. (2018). Internet Gaming Disorder in adolescents: Personality, psychopathology and evaluation of a psychological intervention combined with parent psychoeducation. Frontiers in Psychology, 9, 787. https://doi.org/10.3389/fpsyg.2018.00787
- Griffiths, M. D., Kuss, D. J., Billieux, J., & Pontes, H. M. (2016). The evolution of Internet addiction: A global perspective. Addictive Behaviors, 53, 193-195. https://doi.org/10.1016/j.addbeh.2015.11.001
- Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271-299. https://doi.org/10.1037/1089-2680.2.3.271
- Han, J., Seo, Y., Hwang, H., Kim, S. M., & Han, D. H. (2020). Efficacy of cognitive behavioural therapy for Internet Gaming Disorder. Clinical Psychology and Psychotherapy, 27(2), 203-213. https://doi.org/10.1002/cpp.2419
- Harscoet, V., Hofer, C., Rusinek, S., & Imrani, S. (2013). Thérapie comportementale et cognitive d’un trouble d’anxiété sociale chez une adolescente de culture arabo-musulmane migrante en France. Journal de Thérapie Comportementale et Cognitive, 23(3), 132-141. https://doi.org/10.1016/j.jtcc.2013.06.005
- Haug, S., Castro, R. P., Wenger, A., & Schaub, M. P. (2020). Efficacy of a smartphone-based coaching program for addiction prevention among apprentices: Study protocol of a cluster-randomised controlled trial. BMC Public Health, 20(1), 1910. https://doi.org/10.1186/s12889-020-09995-6
- Imrani, S., & Touri, B. (2025). Adaptation and validation of Moroccan dialect compulsive Internet Use Scale: Validity and reliability. International Journal of Body, Mind and Culture, 12(2), 175-187. https://doi.org/10.61838/ijbmc.v12i2.953
- Karakose, T., Tülübaş, T., & Papadakis, S. (2022). Revealing the intellectual structure and evolution of digital addiction research: An integrated bibliometric and science mapping approach. International Journal of Environmental Research and Public Health, 19(22), 14883. https://doi.org/10.3390/ijerph192214883
- Kim, D., Lee, E., Dong-Min, K. (2008). Development of Internet Addiction Proneness Scale-Short Form(KS scale). Korea Journal of Counseling, 9(4), 1703-1722. https://doi.org/10.15703/kjc.9.4.200812.1703
- Kim, D., Lee, Y., Lee, J., Nam, J. K., & Chung, Y. (2014). Development of Korean smartphone addiction proneness scale for youth. PLoS One, 9(5), e97920. https://doi.org/10.1371/journal.pone.0097920
- Kim, J., Y.-S., Shin, Y.-T., Lim, S.-H., & Seo, J.-W. (2018). A preliminary study on the effectiveness of the peer relationship enhancement program in adolescents at risk for Internet and smartphone addiction. Journal of Child & Adolescent Psychiatry, 29(2), 40-46. https://doi.org/10.5765/jkacap.2018.29.2.40
- Kor, A., & Shoshani, A. (2023). Moderating the impact of the COVID-19 pandemic on children’s and adolescents’ substance use, digital media use, and mental health: A randomized positive psychology addiction prevention program. Addictive Behaviors, 141, 107660. https://doi.org/10.1016/j.addbeh.2023.107660
- Kuss, D. J., & Lopez-Fernandez, O. (2016). Internet addiction and problematic Internet use: A systematic review of clinical research. World Journal of Psychiatry, 6(1), 143-176. https://doi.org/10.5498/wjp.v6.i1.143
- Laconi, S., Rodgers, R. F., & Chabrol, H. (2014). The measurement of Internet addiction: A critical review of existing scales and their psychometric properties. Computers in Human Behavior, 41, 190-202. https://doi.org/10.1016/j.chb.2014.09.026
- Lee, H., Seo, M. J., & Choi, T. Y. (2016). The effect of home-based daily journal writing in Korean adolescents with smartphone addiction. Journal of Korean Medical Science, 31(5), 764-769. https://doi.org/10.3346/jkms.2016.31.5.764
- Lin, Y.-H., Lin, P.-H., Chiang, C.-L., Lee, Y.-H., Yang, C. C. H., Kuo, T. B. J., & Lin, S.-H. (2017). Incorporation of mobile application (app) measures into the diagnosis of smartphone addiction. Journal of Clinical Psychiatry, 78(7), 866-872. https://doi.org/10.4088/JCP.15m10310
- Lindenberg, K., Kindt, S., & Szász-Janocha, C. (2020). Internet addiction in adolescents: The PROTECT program for evidence-based prevention and treatment. Springer Nature. https://doi.org/10.1007/978-3-030-43784-8
- Lindenberg, K., Kindt, S., & Szász-Janocha, C. (2022). Effectiveness of cognitive behavioral therapy-based intervention in preventing gaming disorder and unspecified Internet use disorder in adolescents: A cluster randomized clinical trial. JAMA Network Open, 5(2), e2148995. https://doi.org/10.1001/jamanetworkopen.2021.48995
- Lortie, C., & Guitton, M. J. (2013). 2664 - Internet addiction: Actual status of assessment tools. European Psychiatry, 28(S1), 1. https://doi.org/10.1016/S0924-9338(13)77290-0
- Mark, A. E., & Janssen, I. (2008). Relationship between screen time and metabolic syndrome in adolescents. Journal of Public Health, 30(2), 153-160. https://doi.org/10.1093/pubmed/fdn022
- Meerkerk, G.-J., van den Eijnden, R. J. J. M., Franken, I. H. A., & Garretsen, H. F. L. (2010). Is compulsive internet use related to sensitivity to reward and punishment, and impulsivity?. Computers in Human Behavior, 26(4), 729-735. https://doi.org/10.1016/j.chb.2010.01.009
- Meskini, N., Lamtai, M., Chakit, M., El Aameri, M., Sfendla, A., Loukili, N., & Ouahidi, M. L. (2024). The relationship between smartphone overuse, anxiety, and depression among middle school adolescents in the city of Kenitra, Morocco: A cross-sectional study. Middle East Current Psychiatry, 31(1), 75. https://doi.org/10.1186/s43045-024-00466-x
- Nielsen, P., Christensen, M., Henderson, C., Liddle, H. A., Croquette-Krokar, M., Favez, N., & Rigter, H. (2021). Multidimensional family therapy reduces problematic gaming in adolescents: A randomised controlled trial. Journal of Behavioral Addictions, 10(2), 234-243. https://doi.org/10.1556/2006.2021.00022
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Pan, Y.-C., Chiu, Y.-C., & Lin, Y.-H. (2020). Systematic review and meta-analysis of epidemiology of internet addiction. Neuroscience and Biobehavioral Reviews, 118, 612-622. https://doi.org/10.1016/j.neubiorev.2020.08.013
- Petry, N. M., & O’Brien, C. P. (2013). Internet gaming disorder and the DSM-5. Addiction (Abingdon, England), 108(7), 1186-1187. https://doi.org/10.1111/add.12162
- Pontes, D. H. (2014). The Internet gaming disorder test (IGD-20 test). https://www.halleypontes.com/tests/igd20-test/.
- Reckers-Droog, V., Goorden, M., Kaminer, Y., van Domburgh, L., Brouwer, W., & Hakkaart-van Roijen, L. (2020). Presentation and validation of the Abbreviated Self Completion Teen-Addiction Severity Index (ASC T-ASI): A preference-based measure for use in health-economic evaluations. PLoS One, 15(9), e0238858. https://doi.org/10.1371/journal.pone.0238858
- Rehbein, F., Kliem, S., Baier, D., Mößle, T., & Petry, N. M. (2015). Prevalence of internet gaming disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction (Abingdon, England), 110(5), 842-851. https://doi.org/10.1111/add.12849
- Schneider, L. A., King, D. L., & Delfabbro, P. H. (2017). Family factors in adolescent problematic Internet gaming: A systematic review. Journal of Behavioral Addictions, 6(3), 321-333. https://doi.org/10.1556/2006.6.2017.035
- Shapira, N. A., Lessig, M. C., Goldsmith, T. D., Szabo, S. T., Lazoritz, M., Gold, M. S., & Stein, D. J. (2003). Problematic internet use: Proposed classification and diagnostic criteria. Depression and Anxiety, 17(4), 207-216. https://doi.org/10.1002/da.10094
- Shin, Y.-B., Kim, J.-J., Kim, H., Kim, S.-J., Eom, H., Jung, Y. H., & Kim, E. (2021). Managing game-related conflict with parents of young adults with Internet Gaming Disorder: Development and feasibility study of a virtual reality app. JMIR Serious Games, 9(1), e22494. https://doi.org/10.2196/22494
- Şimşek, N., Zincir, H., Özen, B., & Ceyhan, Ö. (2019). The association between Internet addiction and impulsivity among academicians. Addicta: The Turkish Journal on Addictions, 6(2), 269-281. https://doi.org/10.15805/addicta.2019.6.2.0012
- Singh, A., & Singh, P. (2019). Recent Trends, Current Research in Cyberpsychology: A literature review. Library Philosophy and Practice.
- Stinchfield, R. (2003). Reliability, validity, and classification accuracy of a measure of DSM-IV diagnostic criteria for pathological gambling. American Journal of Psychiatry, 160(1), 180-182. https://doi.org/10.1176/appi.ajp.160.1.180
- Szász-Janocha, C., Vonderlin, E., & Lindenberg, K. (2021). Treatment outcomes of a CBT-based group intervention for adolescents with Internet use disorders. Journal of Behavioral Addictions, 9(4), 978-989. https://doi.org/10.1556/2006.2020.00089
- Torres-Rodríguez, A., Griffiths, M. D., Carbonell, X., & Oberst, U. (2018). Treatment efficacy of a specialized psychotherapy program for Internet Gaming Disorder. Journal of Behavioral Addictions, 7(4), 939-952. https://doi.org/10.1556/2006.7.2018.111
- World Health Organization. (2024). Teens, screens and mental health. https://www.who.int/europe/news-room/25-09-2024-teens--screens-and-mental-health.
- Young, K. S. (1998). Caught in the net: How to recognize the signs of Internet addiction-And a winning strategy for recovery. John Wiley & Sons.
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.