Abstract
The study aims to examine the effect of the motivational interviewing intervention on smoking cessation decisions among university students in Türkiye. The study was conducted with the participation of 64 firstyear university students (experimental group 32, control group 32) who were smokers and wanted to quit. Motivational interviews were completed with students in the experimental group based on quitting smoking (first interview, first month, and third month). Data collection comprised the first interview and the interviews on the first, third, and sixth months, performed on the experimental and control groups using five scales. The team determined that the smoking cessation rate of the students in the experimental group (37.6%) was four times higher than that of the control group (9.4%). A significant difference was found when comparing the smoking cessation status of students according to the follow-ups in the experimental and control groups. In the study, students in the experimental group progressed toward moving to the next stage in the stages of behavior change, aiming at smoking cessation. In contrast, in the control group, there were reversals. Motivational interviewing increases students’ smoking cessation rates and provides positive progress in the stages of behavior change, aiming at smoking cessation.
Keywords: motivational interviewing, nurse, smoking cessation, student
Main Points
- Motivational interviewing increases students’ smoking cessation rates and provides positive progress in the stages of behavior change, aiming at smoking cessation.
- The cessation rate of the experimental group who underwent motivational interviewing was four times higher than that of the control group.
- In the study, students in the experimental group progressed toward moving to the next stage in the stages of behavior change, aiming at smoking cessation, while in the control group, there were reversals.
Introduction
According to the World Health Organization (WHO, 2020), tobacco use is a public health problem that causes the preventable death of over eight million people in the world every year (WHO, 2020). The disease burden of this problem, which is an inducer of non-communicable but early preventable diseases, is greater than that of many epidemics. Many diseases, particularly respiratory diseases, are more severe in individuals due to smoking and exposure to passive smoking, which negatively affects health. It is reported that about a billion people will die in the 21st century due to the use of tobacco and its products if urgent measures are not taken to prevent, reduce, and stop their use (Hsu et al., 2020; WHO, 2020). About 1.2 billion people over the age of 15 worldwide and 19.2 million people in Türkiye use tobacco products. According to the data from the Türkiye Health Survey, the rate of daily tobacco smokers increased from 26.5% in 2016 to 28% in 2019 in individuals aged 15 years and older (Turkish Statistical Institute, 2020). The rate of smoking is also increasing in the young population. In studies conducted with university students in Türkiye, it has been found that smoking rates vary between 25% and 60% (Merih et al., 2021).
The university years are a new physical, social, emotional, and intellectual period in which the transition to young adulthood and cognitive, social, and emotional changes are experienced. During this period, young people may prefer smoking, alcohol, and substance use as coping methods. For this reason, young people are at risk in terms of addictive substance use, and studies on prevention and cessation are necessary (WHO, 2020).
It is observed that more than half of smokers globally want to quit smoking, but their cessation rate is low, between 3% and 12% (Asma et al., 2015; O’Leary & Polosa, 2020). There is great importance in interventions for smoking cessation in all accessible areas in terms of protecting and improving the health of young people, who are more reluctant to seek and request treatment for quitting smoking than adults (Müssener et al., 2016; Pardavila-Belio et al., 2019; WHO, 2020). In addition to pharmacological treatment during the cessation process, initiatives to ensure behavioral changes in individuals increase smoking cessation rates (Ögel & Şimşek, 2021; Sayed et al., 2023; Terzi et al., 2019; Terzi et al., 2023; WHO, 2020).
The trans-theoretical model (TTM) is an integrative, biopsychosocial model used to conceptualize the intentional behavior change process and ensures that the individual is ready to act on healthy behavior (Prochaska & Norcross, 2018). It is important to determine the individual’s stages of behavior change in the model (He et al., 2022).
Motivational interviewing (MI) is an individual method that helps to solve the problem by revealing ambivalence (conflicting emotions) for behavior change. It is necessary to focus on a person’s actions rather than on his words because a person may say that he wants to quit smoking, but he cannot take action (Prochaska & Norcross, 2018; Ögel & Şimşek, 2021). The failure of treatment attempts that force the user to quit addiction reveals the importance of MI and allows people to understand their problems and take action for change (Kumar et al., 2022). The meta-analysis of MI on smoking cessation in university students worldwide determined that MI is positively effective in smoking cessation (Dereli et al., 2023). In MI, the interviewer and the counselee need to move forward together for the commencement and continuity of change.
Lindson-Hawley et al. (2015) stated that, according to the studies they examined on smoking habits, the MI intervention performed by physicians, nurses, and psychological counselors in the form of different sessions provides a high rate of smoking cessation compared to procedural treatment and brief information transfers. From a public health perspective, health personnel, especially public health nurses working in primary health care institutions and school health nurses in educational institutions, have important duties to protect and improve the health of individuals and society (WHO, 2020; Kumar et al., 2022). It has been determined that the professional knowledge and skills of the MI interviewer, as well as the knowledge and competencies related to MI techniques and applications, are more effective in creating behavioral change (Ögel & Şimşek, 2021).
In addition to MI, an effective method for behavior change, and the assessment of young people’s smoking rate status, individual-specific behavioral treatments and interviews should be conducted. Although the necessity and importance of conducting studies aimed at the young population in the fight against tobacco are emphasized, interventional studies aimed at quitting are limited. It was observed that next to the motivational interview for young people to give up smoking, support is provided in the form of educational materials such as brochures and booklets, mobile text messages, and mobile apps (Sayed et al., 2023; Gill et al., 2022; Müssener et al., 2016; Pardavila-Belio et al., 2019; Taş et al., 2016). While examining the multiple and different applications identified in the literature, the lack of a study that only examines the effect of MI stands out, a case that Lindson et al. (2019) also highlighted.
Study Aim
This study aimed to examine the effect of individual motivational interviews applied by a public health nurse to university students who smoke on their decisions to quit smoking.
Material and Methods
Design
This study is a semi-experimental, randomized controlled, open-label interventional study conducted to analyze the effectiveness of MI on smoking cessation decisions in university students.
Participants did not have any information about whether they were included in the experimental or control group. Group assignment was made by the research team using a random number table, and this information was not provided to the participants. The form of the interviews (duration, environment, content structure) was standardized; thus, motivational interviews applied to the experimental group were prevented from being distinguished.
Interviews conducted in an online/hybrid environment due to the pandemic process limited the interaction between the groups. Since the experts implementing the study (e.g., nurse researcher) had group knowledge, a blind structure was not possible.
Setting and Sample
The research sample comprised first-year students (N: 4543) enrolled in the 2021 academic year. An announcement was made to first-year students via the İzmir Katip Çelebi University. The sample group comprised students aged 18 years and older who wanted to participate in the study, wanted to quit smoking, had not been diagnosed with depression, and had a low Beck depression score (n:478). Only individuals with a Beck Depression Inventory (BDI) score between 10 and 16, i.e., individuals with mild depression, were included in the study. Individuals with a moderate or severe depression score (BDI ≥ 17), or those with a previous psychiatric diagnosis, were excluded from the study (n:100). Students who took a course from the research team members were also excluded due to influenceability (n:20). In this study, the sample size was calculated based on the difference in self-efficacy scores between the experimental and control groups to evaluate the effect of MI. The calculation was conducted in line with the findings from the pilot study and similar studies in the literature (Gill et al., 2022; Taş et al., 2016). The parameters used in the calculation were as follows:
- Effect size (Cohen’s d): 0.49
This value was determined based on the group means and standard deviations obtained from the pilot study and similar findings reported in the literature. It was considered a medium effect size.
- Significance level (a): 0.05
A standard 5% error margin was preferred for two-tailed hypothesis testing.
- Statistical power (1−ß): 83.83%
This level of power was chosen to reduce the risk of Type 2 error and to increase the likelihood of detecting a statistically significant difference.
The self-efficacy and competence score effect size between the experimental and control groups was calculated using stratified PASS 11 (Power Analysis Sample Size) in 358 students who met all the criteria as 0.49, the margin of error as 0.05, the power as 83.83% and the sample size of each group as n:23 students (Edwards, 1993). However, considering the potential loss of participation and follow-up during the COVID-19 pandemic, n:40 students were included in each group at the beginning of the study. With this increased number, the statistical power was raised to 93.26%. The students included in the study were divided into an experimental and a control group using a simple random sampling technique according to a randomized table of numbers. The students participating in the study were not given group information to ensure blindness. In addition, since the study was conducted during the online learning process, there were no intra-group and inter-group interactions among the students.
Application of the Research and Collection of Data
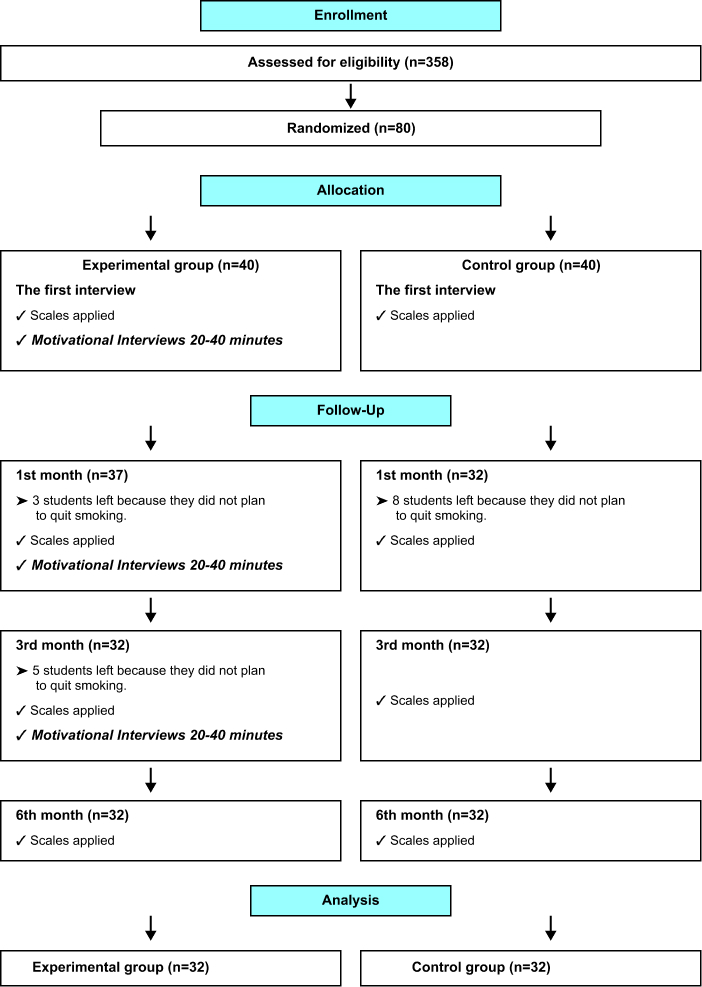
The Consolidated Standards of Reporting Trials flow diagram is shown in Figure 1. Preliminary, first-month, third-month, and sixth-month interviews were conducted with students in the experimental and control groups in the research between April 2021 and December 2021.
In the study, in order to minimize contact between the experimental and control groups, the groups were followed up at different time intervals and in different research environments after random assignment. The interviews were conducted online (on the Zoom platform) and face-to-face with a hybrid interview method in line with the feasibility of education and training during the pandemic. Intervention interviews were conducted individually and confidentially for the experimental group, while only standard information was provided to the control group. Therefore, the control group can be classified as a passive waiting list condition. In addition, students participating in the study were asked not to share the content and processes of the research with other participants. Participants were included in the study within an institutional framework, but all external variables could not be fully controlled. Non-intervention interactions (e.g., out-of-group information, social influences) were tried to be reduced.
Individual motivational interviews based on the behavior change model (MI) (each interview lasted 20–40 minutes on average) were applied to the students in the experimental group. The MIs were planned and implemented according to the stages of change to increase students’ motivation. According to the stages of change, the perception of the importance of quitting smoking, the individual’s belief in the possibility of change, were tried to be strengthened, and a quit plan was made. The interviews were conducted by an academic researcher who was trained in MI, using the OARS technique (Open-ended questions, Affirmation, Reflective listening, and Summarization) together with the stages of change model (Prochaska & Norcross, 2018). The programme encompassed the following areas: the establishment of interpersonal relationships and the cultivation of trust; the identification of conflicts; the assessment of the level of readiness for change; the promotion of change discourse; the establishment of objectives and planning; and the enhancement of self-sufficiency. In order to ensure that the interviews were conducted in accordance with the principles of MI, a structured interview form was employed, and regular supervision was provided throughout the process.
In the intervention group, individual motivational interviews were scheduled at mutually convenient times between the researcher and the participants. The initial session was followed by hybrid (online and face-to-face) follow-up interviews at the first, third, and sixth months, during which relapse episodes and behavioral changes were evaluated using the Stages of Change Short Form. The timeline of the counseling program for the intervention group is shown in Table 1. No intervention or contact beyond routine assessments was provided to the control group.
| Table 1. Timeline of the intervention group counseling program | ||
| Interviews | Counseling and Duration | Consulting Initiative Components |
| The first interview |
Individual online counseling/motivational interview: 20–40 min |
Determination of smoking habit, individual interview in accordance with the change phase, smoking cessation counseling, and application of scales |
| First month |
Individual online counseling/motivational interview: 20–40 min |
Individual interview in accordance with the change phase, smoking cessation counseling, and application of scales |
| Third month |
Individual hybrid (online and face-to-face) counseling/motivational interview: 20–40 min |
Individual interview in accordance with the change phase, smoking cessation counseling, and application of scales |
| Sixth month | Individual face-to-face meeting: 20 min | Determination of smoking status, smoking cessation counseling, and application of scales |
Research data were collected from experimental and control groups using the Student Introduction Form, Beck Depression Inventory, the Fagerström Test for Nicotine Dependence, Sherer’s General Self-Efficacy Scale, the decisional balance measure, Behavior Change Stage Diagnostic Short Question Form, and the Questionnaire of Smoking Urges.
After the interviews started, eight students in the experimental group and eight students in the control group left the study due to giving up on smoking cessation. The study was completed with 64 volunteers who met the participation criteria, 32 of them being in the experimental group and 32 in the control group (Figure 1).
Data Collection Forms
Student Introduction Form
The research team compiled a 17-question form using the relevant literature (Taş et al., 2016; Müssener et al., 2016; Terzi et al., 2019; and Hezer & Karalezli, 2019) to inquire about the student’s sociodemographic characteristics such as age, gender, marital status, department, physiological and spiritual health, medicine use status, age of smoking initiation, smoking habits in the close circle of family and friends, amount of smoking, smoking cessation trial status, the last date of smoking cessation, the longest period of smoking cessation, and previous support for smoking cessation.
Beck Depression Inventory
The BDI was developed by Beck et al. (1961) to assess the somatic, emotional, cognitive, and motivational symptoms of depression. The Turkish adaptation of the scale was conducted by Hisli (1989). The BDI is a self-report inventory consisting of 21 items. Each item is scored on a scale ranging from 0 to 3, yielding a total score that ranges between 0 and 63. Based on the total score, depression severity is classified as minimal depression (0–9 points), mild depression (10–16 points), moderate depression (17–29 points), and severe depression (30–63 points).
The Fagerström Test for Nicotine Dependence
Accurate determination of the individual’s nicotine addiction level is an important factor in increasing the success of smoking cessation attempts. For this purpose, in the evaluation of smoking addiction, the Fagerström Test for Nicotine Dependence (FTND), created by Heatherton et al. (1991) examines the level of an individual’s ability to stay smoke-free for a certain period and the number of cigarettes they smoke. The test consists of six questions, and the score for each question is given separately. According to the results of this test, nicotine addiction is minimal for scores 0–4, moderate for scores 5–6, and high for scores 7–10. In Türkiye, FTND was adapted to Turkish by Uysal et al. (2004), and its reliability and validity were established.
Sherer’s General Self-Efficacy Scale
It is a scale created by Sherer et al. (1982), adapted to Turkish by Gözüm and Aksayan (1999), and developed to evaluate behavior and behavioral changes. In a 5-point Likert-type scale comprising 23 items, each item is marked as 1 - Does not define me at all, 2 - Defines me a little, 3 - I am indecisive, 4 - Defines me well, 5 - Defines me very well. The minimum score is 23, and the maximum score is 115. As the total score obtained from the scale increases, the individual’s perception of self-efficacy also increases.
The Decisional Balance Measure for Assessing and Predicting Smoking Status
The Smoking Decisional Balance Scale explains the benefits and harms of changing problem behavior, in other words, the benefits of change and the obstacles to change. This scale also reveals the cognitive and motivational factors in decision-making. The scale, developed by Velicer et al. (1985), had its validity and reliability established by Plummer et al. (2001). The adaptation of the scale to Turkish society was made by Yalçınkaya-Alkar and Karanci (2007). The scale comprises 24 items, 12 items measuring the perceived positive aspects of smoking and 12 items measuring the perceived negative aspects of smoking. In the scale scored in the Likert style, the items are evaluated between 1 and 5 (1 - Completely disagree, 2 - Disagree, 3 - Indecisive, 4 - Agree, 5 - Completely agree). The lowest score was 12, and the highest score was 60 in the dimension of perceived benefits and perceived harms of smoking. The overall average score of the scale is obtained by subtracting the perceived benefits from the perceived harms of the smoking score. The fact that the overall average score of the scale has a negative value indicates that the perceived harms of smoking predominate, while the fact that it has a positive value indicates that the perceived benefits of smoking predominate.
Behavior Change Stage Diagnostic Short Question Form
The change questions developed by DiClemente et al. (1991) enable the identification of the stages of change that people who want to change their problematic behavior and strive for it go through. The change phase assessment questions are an algorithm that determines the stages of people thinking about quitting smoking and consists of five stages. The individuals participating in the study are asked to choose one of the options that match the behavior change stage levels for smoking cessation. The answer of an individual to the “Have you stopped smoking?” question determines the stage of change. These stages and their corresponding answers are:
- Pre-contemplation: “I’m not thinking of quitting in the next 6 months.”
- Contemplation: “I’m thinking of quitting in 6 months.”
- Preparation: “I’m thinking of quitting in 30 days.”
- Action: “I quit less than 6 months ago.”
- Maintenance: “I quit more than 6 months ago” (Velicer et al., 1998).
The Questionnaire of Smoking Urges
The validity and reliability study of the Questionnaire of Smoking Urges was conducted by Demirezen (2013). The scale is rated between 1 -- strongly disagree at all, 2 - disagree, 3 - partially disagree, 4 - indecisive, 5 - partially agree, 6 - agree, and 7 - strongly agree in the Likert-type and contains ten questions. The lowest score on the scale is 10, which indicates that there is no desire to smoke. The highest score is 70, which indicates a very high desire to smoke.
The Ethical Approval of the Research
Ethical committee approval was received from the Ethics Committee of İzmir Katip Çelebi University Non-Interventional Clinical Studies (Approval no: 1071; Date: November 19, 2020). For the scales used in the research, permissions were obtained from the scale owners. The purpose of the research was explained, and an online consent form and verbal permission were obtained from the students participating in the research. The Clinical Trial registration of the study was completed (NCT05324644).
Data Analysis
In data analysis, the team used the SPSS for Windows version 25.0 (IBM SPSS Corp.; Armonk, NY, USA). Mean ± standard deviation, median (maximum-minimum), percentage, and frequency values were used for the variables. The validity of the repeated measures of the data for analysis of variance was evaluated by Mauchly’s sphericity test and the Box-M homogeneity test of variances. In order to compare the averages, a factorial repeated measures analysis of variance was used. One of the Greenhouse and Geisser (1959) or Huynh and Feldt (1976) tests was used to correct the degrees of freedom that did not meet the prerequisites of parametric tests (a factorial repeated measures analysis of variance). Multiple comparisons were performed with the Corrected Bonferroni Test (Edwards, 1993).
The normality of the variables and the homogeneity of the variances were evaluated after checking the prerequisites (Shapiro–Wilk and Levene Test). While performing data analysis, for the comparison of two groups, the Mann–Whitney U test was used, and for the comparison of three or more groups, ANOVA and repeated measures analysis of variance were used. Categorical data were analyzed by Fisher’s exact test and chi-square test. In cases where the expected frequencies are less than 20%, the “Monte Carlo Simulation” method was used to evaluate the inclusion of these frequencies in the analysis. p < .05 and p < .01 were accepted for the significance level of the tests.
Results
Participant Characteristics
While comparing the distribution of students in the experimental and control groups according to their sociodemographic characteristics, it was determined that the groups were similar, and that there was no difference between their age, gender, department of studies, history of illness, or drug use status (p > .05).
The Smoking Status of Students
Students in the experimental and control groups were not different regarding their age of smoking initiation, average monthly expense for tobacco products, smoking habits in the close circle of family and friends, amount of smoking, usage of other addictive substances, smoking cessation trial status, and previous support for smoking cessation (p > .05).
Depression Status of the Students
At the beginning of the study, the mean BDI score of the students in the experimental group was found to be 11.21 ± 4.69, while that of the control group was found to be 11.90 ± 4.69. Both groups were in the mild depression category, and no statistically significant difference was found between the groups (p > .05).
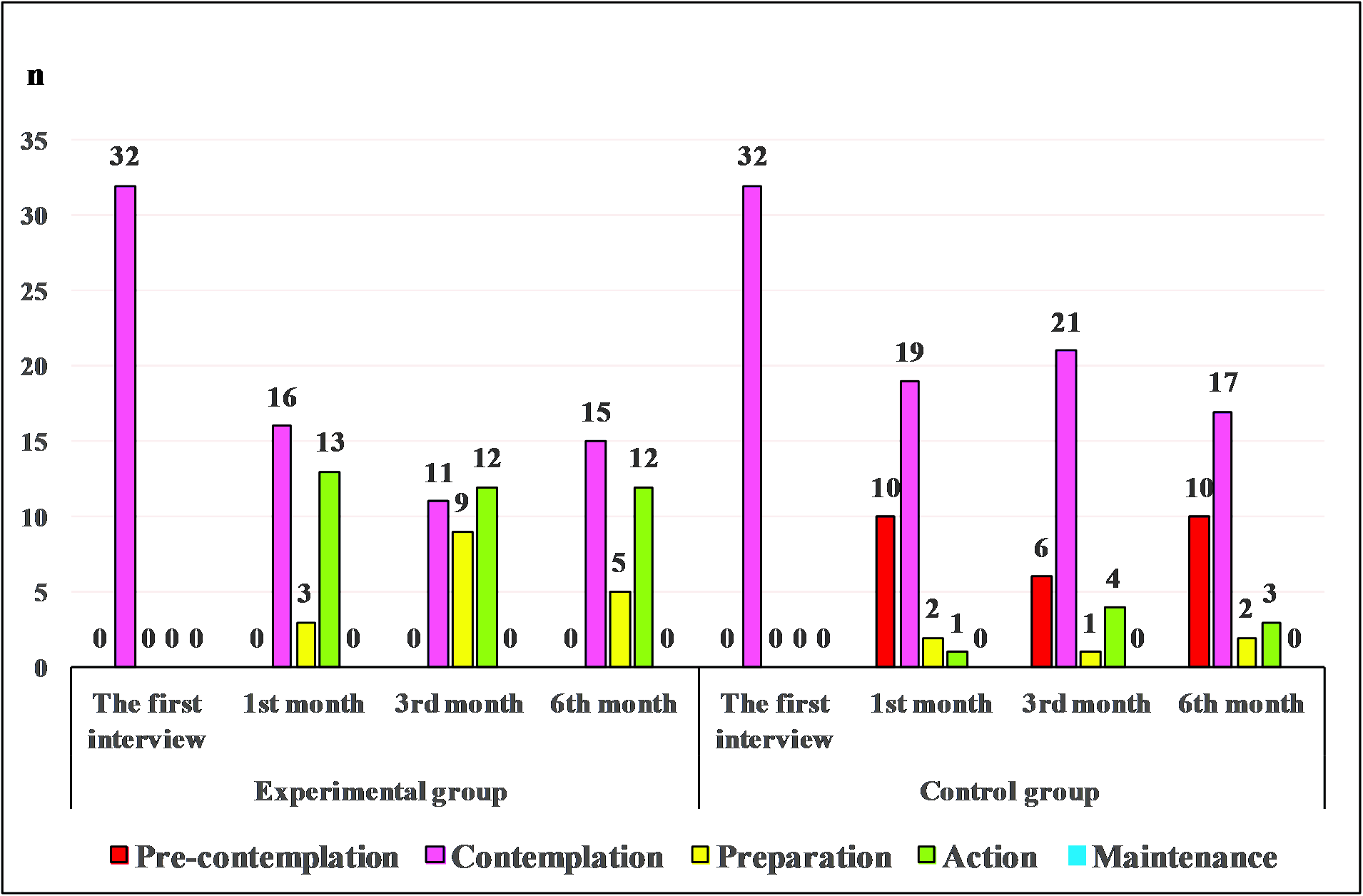
The Distribution of Students’ Behavior Change Stages According to Repeated Measurements
During the sixth month interview, it was detected that from the students of the experimental group who conducted motivational interviews, 46.9% (n = 15) of them were at the contemplation stage, 15.6% (n = 5) were at the preparation stage, and 37.5% (n = 12) were at the action stage, while from the students of the control group, 31.3% (n = 10) of them were at the pre-contemplation stage, 53.1% (n = 17) were at the contemplation stage, 6.3% (n = 2) were at the preparation stage, and 9.4% (n = 3) were at the action stage (Figure 2).
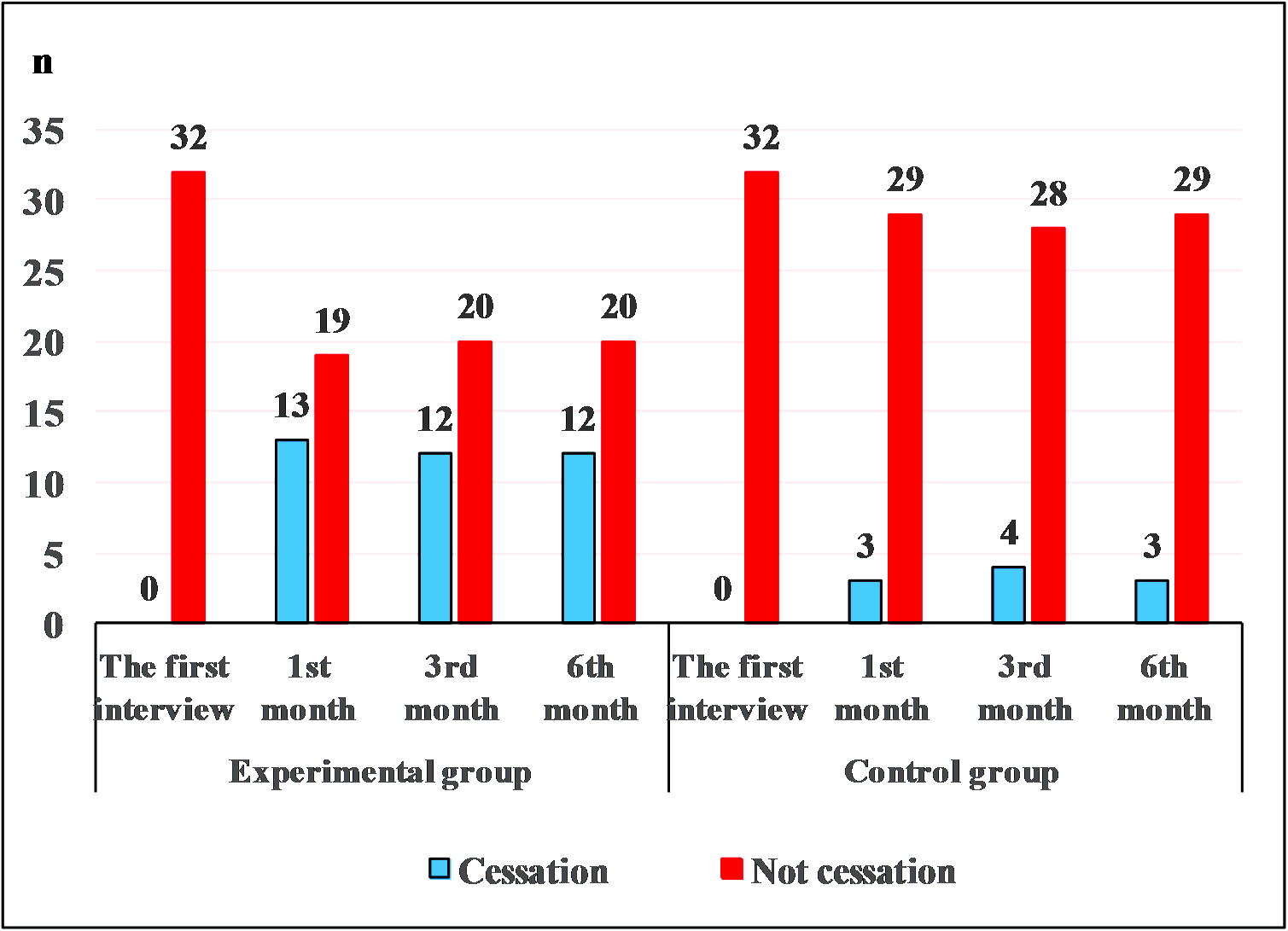
The Comparison of Students’ Smoking Cessation Status According to Repeated Measurements
The smoking cessation rate of the students in the experimental group (37.5%; n:12) was four times higher than that of the control group (9.4%; n:3) during the sixth month (Figure 3). There was a significant difference in the comparison of the smoking cessation status of students in the experimental and control groups according to the follow-ups (p < .05) (Figure 3).
The Comparison of the Fagerström Test for Nicotine Dependence, Sherer’s General Self-Efficacy Scale, the Decisional Balance Measure for Assessing and Predicting Smoking Status, and the Questionnaire of Smoking Urges Score Averages of Students in Experimental and Control Groups According to Repeated Measurements
The comparison of FTND scores in repeated measurements between groups showed no significant difference in the first interview (p = .440) and the follow-ups of the first month (p = .086) and sixth month (p = 0.252), but detected a significant difference in the third month interview (p < .05). In the experimental group where MI was applied, the FTND values of the students who were at the intermediate level (5.15 ± 1.32) at the first interview decreased to a low level (3.50 ± 1.93) at the end of the third month. A significant difference was found in the comparison of the mean FTND scores of the students in the experimental and control groups according to the time-dependent follow-ups (p < .001) (Table 2).
| Table 2. The comparison of the score averages of students in experimental and control groups according to repeated measurements (n: 64) | |||||||
| Scales | Groups |
|
|
|
|||
|
|
|
|
|
||||

|
|
|
|
||||
| FTND | Experimental |
|
|
|
|
|
|
| Control |
|
|
|
|
|
|
|
| Test statistic ** |
|
|
|
|
|||
| p |
|
|
|
|
|||
| SGSES | Experimental |
|
|
|
|
|
|
| Control |
|
|
|
|
|
|
|
| Test statistic ** |
|
|
|
|
|||
| p |
|
|
|
|
|||
| DBM | Experimental |
|
|
|
|
|
|
| Control |
|
|
|
|
|
|
|
| Test statistic ** |
|
|
|
|
|||
| p |
|
|
|
|
|||
| QSU | Experimental |
|
|
|
|
|
|
| Control |
|
|
|
|
|
|
|
| Test statistic ** |
|
|
|
|
|||
| p |
|
|
|
|
|||
|
The p-values in bold represent statistical difference. Note: DBM = Decisional balance measure; FTND = Fagerström test for nicotine dependence; n = Number; QSU = Questionnaire of Smoking Urges; SGSES = Sherer’s General Self-Efficacy Scale; ss = Standard deviation; X = Mean. 
*Time-dependent repeated analysis of variance test. **Group-dependent repeated analysis of variance test. |
|||||||
There was no significant difference between the groups’ SGSES total score averages (p > .05) {(first (p = .142), first month (p = .946), third month (p = .190), and sixth month (p = .630) interviews}. According to the repeated measurements made on the students in the experimental and control groups, their SGSES scores decreased, and a significant time-related difference was found (p < .05) (Table 2).
While examining the students’ decisional balance measure (DBM) scores, it was determined that the perceived harms of smoking were higher in the experimental group (−15.03 ± 11.06) than in the control group (−8.06 ± 11.06). While there was no significant difference in the DBM scores of the first (p = .184), first month (p = .208), and third month (p = .056) interviews (p > .05), a significant difference was found in the sixth-month interview (p = .014) (p < .05). There was no significant time-related difference in the repeated measurement of the experimental and control groups’ DBM scores (p > .05) (Table 2).
While comparing the students’ average scores of QSU, the experimental group’s scores were lower in all interviews compared to the control group, and there was no significant difference between the first (p = .438), first month (p = .530), third month (p = .084), and sixth month (p = .186) interviews. There was no significant time-related difference in the average repeated measurement of QSU scores in the experimental and control groups (p > .05) (Table 2).
Discussion
In the research, the effect of MI on students’ decisions toward smoking cessation was examined. Changes in smoking cessation rates and behavioral stages in the study showed that MI is effective in quitting smoking, and the results are consistent with other studies (Taş et al., 2016; Müssener et al., 2016; Terzi et al., 2019; Arslanoğlu et al., 2020; Merih et al., 2021; Brar et al., 2020; Deressa Guracho et al., 2020; Gill et al., 2022; Nasser et al., 2020; Xiong et al., 2020; Zeng et al., 2020; Sayed et al., 2023; Dereli et al., 2023).
The cessation rate of the experimental group (37.6%) who underwent MI was found to be four times higher than that of the control group (9.4%). The cessation rates of the studies with MI application vary in a broad range (14% in Pardavila-Belio et al., 2019; 16.5% in Gill et al., 2022; 20.6% in Müssener et al., 2016; 21.1% in Pardavila-Belio et al., 2015; 33.3% in Erol and Erdoğan, 2008; 37% in Güngörmüş and Erci, 2012; 46.1% in Taş, 2015; 69.1% in Karadağ et al., 2011; 80.5% in Sayed et al., 2023). This wide range is thought to be due to the application of text messages, training, and applications that support quitting similar to MI in other studies. This study has only determined the effectiveness of MI, and similar further studies will be useful in determining the effectiveness of MI more clearly.
At the end of the sixth month, 17 participants in the experimental group were in the preparation and action stages, indicating progress in the behavior change stages, while 10 participants in the control group with no MI application returned to the pre-contemplation stage. This situation shows that MI affects the behavior change stages of students’ smoking cessation decisions and that there are advances from the contemplation stage to the action stage. Similar findings have been highlighted in other studies (Durmaz et al., 2019; Gill et al., 2022; Taş et al., 2016; Terzi et al., 2019; Pardavila-Belio et al., 2019; Sayed et al., 2023). Lindson-Hawley et al. (2015), in their meta-analysis studies, found that MI by primary care physicians, nurses, or counselors, in the procedure of one to six sessions, with a session duration varying from 10 to 60 minutes, is effective in behavior change. Dereli et al. (2023), in a meta-analysis, reported that MI is effective in promoting smoking cessation among university students.
In the study, the initial FTND medium and low scores decreased as the students’ stages of change progressed, and there have been similar results in many other studies conducted on the young population (Brar et al., 2020; Deressa Guracho et al., 2020; Kim et al., 2018; Nasser et al., 2020; Xiong et al., 2020; Zeng et al., 2020; Arslanoğlu et al., 2020; Durmaz et al., 2019; Merih et al., 2021; Sözer et al., 2021; Terzi et al., 2019). The FTND score is an effective indicator of behavior change and cessation rate in cessation attempts (Pardavila-Belio et al., 2019; Hezer & Karalezli, 2019; Gill et al., 2022). For this reason, the relevant university units should determine and record the students’ smoking status and conduct short MI for smoking cessation.
The smoking cessation rates of the experimental group at the end of the sixth month were higher than those of the control group. However, contrary to expectations, there was a decrease in the SGSES scores of the students in the experimental group, showing no significant difference between the experimental and control groups.
Individuals demonstrating higher levels of self-efficacy are more likely to continue progressing through the action and maintenance stages. This is attributable to the fact that self-efficacy has been reported to be associated with behavioral change. This underscores the pivotal function of self-efficacy in maintaining long-term behavioral modifications (Karl, 2020; Pardavila-Belio et al., 2019). The observed variations in self-efficacy scale scores can be ascribed to the unique conditions engendered by the pandemic. The pandemic may have exerted its influence on levels of self-efficacy through a variety of mechanisms. It is hypothesised that restrictions on social interaction, limited access to support systems, disruptions in daily routines, and increased psychological stress may have undermined individuals’ confidence in initiating or sustaining behavioral changes. Conversely, for some individuals, heightened health concerns during the pandemic may have functioned as a catalyst for motivation, thereby reinforcing commitment to change and augmenting self-efficacy.
The decline in DBM scores observed in the experimental group following the implementation of an MI intervention suggests an enhancement in awareness regarding the adverse consequences associated with smoking. Furthermore, the finding that the experimental group’s DBM scores were significantly lower than those of the control group (p < .05) suggests that MI may have effectively changed participants’ cognitive assessments of the costs and benefits of smoking. This shift in decision balance is indicative of an increased awareness of the health risks and social consequences of smoking, thereby facilitating progress toward behavioral change.
These findings are consistent with previous research showing that increasing awareness of both the benefits and harms of problematic behaviors strengthens individuals’ motivation to change (Yararbaş et al., 2019). Within the framework of MI, decision balance plays an important role by creating ambivalence in the individual. Indecision constitutes a fundamental element targeted therapeutically in MI, helping individuals resolve internal conflicts and progress through the stages of change. As indecision decreases and the negative aspects of smoking become more apparent, individuals are more likely to progress from the contemplation stage to the preparation stage and ultimately to the action and maintenance stages.
Consequently, evaluating individuals’ perceptions of the advantages and disadvantages of smoking can serve not only as a diagnostic instrument but also as an effective component in the tailoring of MI sessions to the individual. This approach has the potential to facilitate the development of more targeted interventions, enhanced participant involvement in the process, and ultimately, the promotion of enduring behavioral change in smoking cessation programmes for university students.
Research has identified the craving or urge to smoke as an important predictor of both relapse (re-starting) and difficulties in maintaining smoking cessation (Müssener et al., 2016; Demirezen & Kurçer, 2017; Hezer & Karalezli, 2019). It is therefore evident that the recognition and effective management of cravings is considered a critical component of smoking cessation interventions. It has been demonstrated by preceding studies that MI has the capacity to contribute to a reduction in craving levels by means of an increase in individuals’ intrinsic motivation, the development of their coping skills, and the addressing of their ambivalence toward smoking.
In this study, although the decrease in Cigarette Craving Scale (QSU) scores was not statistically significant (p > .05), a consistent downward trend was observed over time; lower craving scores were recorded in the experimental group compared to the control group at each measurement point. This pattern suggests that MI may have a gradual effect on craving levels, which may have been achieved by strengthening participants’ cognitive control, improving their emotional regulation, and increasing their awareness of internal triggers. The absence of statistical significance may be ascribed to a number of factors, including the comparatively brief follow-up period, the limited sample size, or individual variations in withdrawal symptoms.
It is widely acknowledged that craving represents a significant challenge for individuals attempting to quit smoking, often resulting in relapse during the early stages of the process, as well as during the maintenance phase. In this context, the integration of MI into nursing practices in counseling units may offer an effective approach to coping with withdrawal-related distress. MI employs client-centred and non-confrontational techniques to assist individuals in identifying coping strategies, anticipating high-risk situations, and developing personalised plans for managing urges. This approach is designed to support sustained cessation.
While secondary variables such as self-efficacy, decisional balance, and craving were measured and reported, this study was not designed to examine their mediating roles. Future research with larger sample sizes and structural modeling approaches is recommended to explore how these psychological constructs influence or mediate the process of smoking cessation.
The findings of this study underscore the potential value of incorporating MI into comprehensive smoking cessation programs delivered by nurses, who are often the first point of contact in health care settings and are well-positioned to provide ongoing behavioral support. Future studies employing larger sample sizes and longer follow-up periods may better capture the cumulative effects of MI on craving reduction and long-term abstinence outcomes.
Limitations and Directions/Suggestions for Future Research
The study only conducted analyses on participants who completed the intervention process, and no intention-to-treat (ITT) analysis was performed. This reduces the representativeness of the sample and limits the generalizability of the findings because the effects of individuals who dropped out of the study were not taken into account. In future studies, it is recommended that the ITT approach and appropriate missing data completion methods (e.g., multiple imputation) be used to reduce the effect of missing data. Data on smoking cessation status are based on participants’ self-reports, and objective biochemical verification methods (e.g., cotinine or carbon monoxide measurements) were not used. This may lead to a risk of reporting bias, so caution should be exercised in interpreting the results.
A notable limitation of this study is its open label design, as participants were aware of whether they were receiving online or face-to-face training. This awareness may have introduced expectation bias, performance bias, and social desirability effects.
This study shows that TTM-based MI is effective in students’ smoking cessation decisions and provides progress in the behavior change phase during the smoking cessation process. The strength of the study is that motivational interviews were only conducted for students during the cessation process, eliminating other influences. It is recommended to ensure that students choose their colours to create awareness in all accessible areas, and apply MI using a nurse in smoking cessation therapies. Conducting motivational interviews with a nurse about quitting smoking provides a unique opportunity for students to support their decision to quit smoking. It is proposed to establish units in universities where students who want to quit smoking can apply, receive counseling, and expand the use of MI.
Acknowledgements
We would like to thank the students who participated in this study, the university administration. We would like to thank the Turkish Green Crescent Society.
Ethical approval
This study was approved by the Izmir Katip Celebi University Non-Interventional Clinical Studies Ethical Committee (Date: November 19, 2020, Decision/Protocol No: 1071). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study was supported by the the Green Crescent Graduate Thesis Research Scholarship Support Program under Grant Number 2021-9.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Arslanoğlu, C., Acar, K., Arslanoğlu, E., Baynaz, K., Karakaş, F., İpekoğlu, G., & Mor, A. (2020). Investigation of smoking habits and quality of life of university students (sample of Sinop university). Ekev Akademi Dergisi, 24(84), 195-210. https://doi.org/10.17753/Ekev1753
- Asma, S., Mackay, J., Song, S. Y., Zhao, L., Morton, J., & Palipudi, K. M. (2015). The GATS Atlas: Global Adult Tobacco Survey. CDC Foundation. Centers for Disease Control and Prevention; World Lung Foundation; Global Tobacco Surveillance System; World Health Organization.
- Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry, 4(6), 561-571. https://doi.org/10.1001/archpsyc.1961.01710120031004
- Brar, M., Chaudhary, N., Ramakrishnan, T. S., & Randhawa, A. (2020). A study of prevalence of tobacco use and related factors among medical students as per the Global Health Professions Student Survey protocol. International Journal of Research in Medical Sciences, 8(6), 2243-2247. https://doi.org/10.18203/2320-6012.ijrms20202275
- Demirezen, M. (2013). Sigara içme arzusu ölçeği’nin Türkçe geçerlilik, güvenilirliği ve anksiyete ile ilişkisi (Thesis No. 340747) [Medical specialization thesis, Bülent Ecevit University]. Council of Higher Education National Thesis Center.
- Demirezen, M., & Kurçer, M. A. (2017). Effect of smoking cessation on anxiety and urge for smoking. Journal of Dependence, 18(2), 53-58.
- Dereli, F., Tekindal, M., & Agah Tekindal, M. A. (2023). The effect of motivational interviewing on smoking cessation of university students: A meta-analysis. ADDICTA: The Turkish Journal on Addictions, 10(3), 275-281. https://doi.org/10.5152/ADDICTA.2023.23138
- Deressa Guracho, Y., Addis, G. S., Tafere, S. M., Hurisa, K., Bifftu, B. B., Goedert, M. H., & Gelaw, Y. M. (2020). Prevalence and factors associated with current cigarette smoking among Ethiopian university students: A systematic review and meta-analysis. Journal of Addiction, 2020, 9483164. https://doi.org/10.1155/2020/9483164
- Diclemente, C. C., Prochaska, J. O., Fairhurst, S., Velicer, W. F., Rossi, J. S., & Velasquez, M. (1991). The process of smoking cessation: An analysis of precontemplation, contemplation and contemplation/action. Journal of Consulting and Clinical Psychology, 59(2), 295-304. https://doi.org/10.1037/0022-006X.59.2.295
- Durmaz, S., Ergin, I., Durusoy, R., Hassoy, H., Caliskan, A., & Okyay, P. (2019). WhatsApp embedded in routine service delivery for smoking cessation: Effects on abstinence rates in a randomized controlled study. BMC Public Health, 19(1), 387. https://doi.org/10.1186/s12889-019-6727-z
- Edwards, L. K. (1993). Applied analysis of variance in the behavioral sciences. Marcel Dekker, Inc.
- Erol, S., & Erdoğan, S. (2008). Application of a stage based motivational interviewing approach to adolescent smoking cessation: The transtheoretical Model-based study. Patient Education and Counseling, 72(1), 42-48. https://doi.org/10.1016/j.pec.2008.01.011
- Gill, V. S., Chaudhary, N., Randhawa, A., Verma, M., Rai, G. K., & Mishra, S. (2022). A prospective study to assess the outcome of motivational interviewing among male students of Haryana, India: A strive towards smoking cessation in the youth. Cureus, 14(2), e22642. https://doi.org/10.7759/cureus.22642
- Gözüm, S., & Aksayan, S. (1999). The reliability and validity of Turkish form of the self-efficacy scale. Journal of Anatolia Nursing and Health Sciences, 2(1), 21-34.
- Greenhouse, S. W., & Geisser, S. (1959). On methods in the analysis of profile data. Psychometrika, 24(2), 95-112. https://doi.org/10.1007/BF02289823
- Güngörmüş, Z., & Erci, B. (2012). Transtheoretical Model -Based education given for smoking cessation in higher school students. Southeast Asian Journal of Tropical Medicine and Public Health, 43(6), 1548-1559.
- He, L., Basar, E., Wiers, R. W., Antheunis, M. L., & Krahmer, E. (2022). Can chatbots help to motivate smoking cessation? A study on the effectiveness of motivational interviewing on engagement and therapeutic alliance. BMC Public Health, 22(1), 726. https://doi.org/10.1186/s12889-022-13115-x
- Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerström, K. O. (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. British Journal of Addiction, 86(9), 1119-1127. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x
- Hezer, H., & Karalezli, A. (2019). The effect of psychological dependence on smoking urge and nicotine withdrawal symptoms. Ankara Medical Journal, 19(4), 700-707. https://doi.org/10.17098/amj.651955
- Hisli, N. (1989). Beck depresyon envanterinin üniversite öğrencileri için geçerliği, güvenirliği. Psikoloji Dergisi, 7(23), 3-13.
- Hsu, C. Y., Liao, H. E., & Huang, L. C. (2020). Exploring smoking cessation behaviors of outpatients in outpatient clinics: Application of the transtheoretical model. Medicine, 99(27), e20971. https://doi.org/10.1097/MD.0000000000020971
- Huynh, H., & Feldt, L. S. (1976). Estimation of the box correction for degrees of freedom from sample data in randomized block and split-plot designs. Journal of Educational Statistics, 1(1), 69-82. https://doi.org/10.3102/10769986001001069
- Karadağ, M., Karadağ, S., Ediz, S., & Işık, E. S. (2011). The effect of nicotine dependence on smoking cessation. New Journal of Medicine, 29(1), 27-31.
- Karl, T. (2020). The 5 stages of change and the Transtheoretical Model (TTM) — Do i know the basics?. https://r1learning.com/blog/2020/5-stages-of-change
- Kim, B., Yoo, S., & Cho, S. I. (2018). Association between stages of change for smoking cessation and electronic cigarette use among adult smokers: A nationwide cross-sectional study in Korea. PLoS One, 13(9), e0204244. https://doi.org/10.1371/journal.pone.0204244
- Kumar, R., Sahu, M., & Rodney, T. (2022). Efficacy of motivational interviewing and brief interventions on tobacco use among healthy adults: A systematic review of randomized controlled trials. Investigacion y Educacion en Enfermeria, 40(3), e03. https://doi.org/10.17533/udea.iee.v40n3e03
- Lindson, N., Thompson, T. P., Ferrey, A., Lambert, J. D., & Aveyard, P. (2019). Motivational interviewing for smoking cessation. Cochrane Database of Systematic Reviews, 7(7), CD00693. https://doi.org/10.1002/14651858.CD006936.pub4
- Lindson-Hawley, N., Thompson, T. P., & Begh, R. (2015). Motivational interviewing for smoking cessation. Cochrane Database of Systematic Reviews, 3(3), CD006936. https://doi.org/10.1002/14651858.CD006936.pub3
- Merih, Y. D., Güdük, Ö., Ertürk, N., Yemenci, M., Arğa, K. Y., & Satman, İ. (2021). Determinants of tobacco use habits and perceptions among university students: A systematic review study. Journal of Health Institutes of Türkiye, 4(1), 49-84.
- Müssener, U., Bendtsen, M., Karlsson, N., White, I. R., McCambridge, J., & Bendtsen, P. (2016). Effectiveness of short message service text-based smoking cessation intervention among university students: A randomized clinical trial. JAMA Internal Medicine, 176(3), 321-328. https://doi.org/10.1001/jamainternmed.2015.8260
- Nasser, A. M., Geng, Y., & Al-Wesabi, S. A. (2020). The prevalence of smoking (cigarette and waterpipe) among university students in some Arab countries: A systematic review. Asian Pacific Journal of Cancer Prevention: APJCP, 21(3), 583-591. https://doi.org/10.31557/APJCP.2020.21.3.583
- O’Leary, R., & Polosa, R. (2020). Tobacco harm reduction in the 21st Century. Drugs and Alcohol Today, 20(3), 219-234. https://doi.org/10.1108/DAT-02-2020-0007
- Ögel, K., & Şimşek, M. (2021). Motivasyonel görüşme tekniği. İş Bankası Kültür Yayınları.
- Pardavila-Belio, M. I., García-Vivar, C., Pimenta, A. M., Canga-Armayor, A., Pueyo-Garrigues, S., & Canga-Armayor, N. (2015). Intervention study for smoking cessation in Spanish college students: Pragmatic randomized controlled trial. Addiction (Abingdon, England), 110(10), 1676-1683. https://doi.org/10.1111/add.13009
- Pardavila-Belio, M. I., Ruiz-Canela, M., & Canga-Armayor, N. (2019). Predictors of smoking cessation among college students in a pragmatic randomized controlled trial. Prevention Science, 20(5), 765-775. https://doi.org/10.1007/s11121-019-01004-6
- Plummer, B. A., Velicer, W. F., Redding, C. A., Prochaska, J. O., Rossi, J. S., Pallonen, U. E., & Meier, K. S. (2001). Stage of change, decisional balance, and temptatios for smoking measurement and validation in a large, school-based population of adolescent. Addictive Behaviors, 26(4), 551-571. https://doi.org/10.1016/s0306-4603(00)00144-1
- Prochaska, J. O., & Norcross, J. C. (2018). Systems of psychotherapy: A transtheoretical analysis. Oxford University Press.
- Sayed, S. H., El-Sakkar, S. M., Ahmed Elsaka, S. A., & El-Houfey, A. A. (2023). Effect of cigarette smoking cessation educational intervention based on trans-theoretical model using motivational interviewing on Egyptian males’ smoking knowledge and behavior: A randomized controlled trial. Nursing Practice Today, 10(2), 108-123. https://doi.org/10.18502/npt.v10i2.12832
- Xiong, P. S., Xiong, M. J., Liu, Z. X., & Liu, Y. (2020). Prevalence of smoking among adolescents in China: An updated systematic review and meta-analysis. Public Health, 182, 26-31. https://doi.org/10.1016/j.puhe.2020.01.011
- Sherer, M., Maddux, J. E., Mercandante, B., Prentice-Dunn, S., Jacobs, B., & Rogers, R. W. (1982). The self-efficacy scale: Construction and validation. Psychological Reports, 51(2), 663-671. https://doi.org/10.2466/pr0.1982.51.2.663
- Sözer, Ü., Özvurmaz, S., & Durmaz, S. (2021). Readiness of healthcare workers to receive support for smoking cessation and related factors. Turkish Journal of Family Medicine and Primary Care, 15(2), 286-293. https://doi.org/10.21763/tjfmpc.782565
- Taş, F. (2015). Lise öğrencilerinde ağızotunu (Dumansız tütün) bıraktırmaya yönelik transteoretik model temelli motivasyonel görüşmelerin etkisi (Thesis No. 408430) [Doctoral dissertation, Erciyes University]. Council of Higher Education National Thesis Center.
- Taş, F., Seviğ, E. Ü., & Güngörmüş, Z. (2016). Use of motivational interview technique with transtheoretical model for behavioral change in smoking addiction. Current Approaches in Psychiatry, 8(4), 380-392. https://doi.org/10.33715/inonusaglik.737711
- Terzi, H., Kitiş, Y., & Akin, B. (2023). Effectiveness of non-pharmacological community-based nursing interventions for smoking cessation in adults: A systematic review. Public Health Nursing, 40(1), 195-207. https://doi.org/10.1111/phn.13132
- Terzi, O., Kumcagiz, H., Terzi, M., & Dundar, C. (2019). Cigarette smoking and determination of nicotine dependence levels in university students. ADDICTA: The Turkish Journal on Addictions, 6(4), 168-181. https://doi.org/10.5152/addicta.2020.19134
- Turkish Statistical Institute. (2020). Global adult tobacco survey. https://data.tuik.gov.tr/Bulten/Index?p=Turkiye-Saglik-Arastirmasi-2019
- Uysal, M. A., Kadakal, F., Karşıdağ, C., Bayram, N. G., Uysal, O., & Yılmaz, V. (2004). Fagerström test for nicotine dependence: Reliability in a Turkish sample and factor analysis. Tüberküloz ve Toraks, 52(2), 115-121.
- Velicer, W. F., DiClemente, C. C., Prochaska, J. O., & Brandenburg, N. (1985). Decisional balance measure for assessing and predicting smoking status. Journal of Personality and Social Psychology, 48(5), 1279-1289. https://doi.org/10.1037//0022-3514.48.5.1279
- Velicer, W. F., Prochaska, J. O., Fava, J. L., Norman, G. J., & Redding, C. A. (1998). Smoking cessation and stress management: Applications of the transtheoretical model. Homeostasis, 38(5-6), 216-233.
- Yalçinkaya-Alkar, O., & Karanci, A. N. (2007). What are the differences in decisional balance and self-efficacy between Turkish smokers in different stages of change?. Addictive Behaviors, 32(4), 836-849. https://doi.org/10.1016/j.addbeh.2006.06.023
- Yararbaş, G., Keles, D. O., Altuner, O. G., Turgut, C. B., Yilmaz, C., & Yuksel, K. (2019). Determination and evaluation of smoking status of individuals under probation. Addicta: The Turkish Journal on Addictions, 6(4), 215-244. https://doi.org/10.5152/addicta.2020.19114
- Zeng, L. N., Zong, Q. Q., Zhang, J. W., An, F. R., Xiang, Y. F., Ng, C. H., Ungvari, G. S., Yang, F. Y., Yan, H., Chen, L. G., Hu, X., & Xiang, Y. T. (2020). Prevalence of smoking in nursing students worldwide: A meta-analysis of observational studies. Nurse Education Today, 84, 104205. https://doi.org/10.1016/j.nedt.2019.104205
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.