Abstract
Caregiver’s attitudes toward recovery of their drug addicted loved one significantly influence their behavioral orientation toward recovery, adherence to treatment procedures, and sustainability of sobriety. There is, however, a lack of any scale for its assessment, and thus the present study aimed to develop and validate the caregiver’s attitudes toward drug addict’s recovery scale. In-depth interviews were conducted with caregivers (N = 17, Mage = 39.35), and interpretative phenomenological analysis was used to generate superordinate themes of beliefs, negative feelings, and active involvement toward recovery. The items for each theme were generated, and after content validity, a pool 44 items was obtained. The factor structure of the scale was determined on a sample of 284 caregivers (Mage = 39.57), resulting in four subscales (i.e., negative recovery expectations, positive recovery expectations, emotional resentment, therapeutic pessimism) explaining 49.01% variance. The construct validity was assessed through confirmatory factor analysis (N = 400, Mage = 43.38), demonstrating good indices of fit for 42 out of 44 items. The convergent and discriminant validity of the retained item pool with scores on internalized stigma demonstrated a significant positive correlation with negative recovery expectations, emotional resentment, and therapeutic pessimism, whereas there was no correlation with positive recovery expectations. The reliability coefficients for subscales ranged from 0.77 to 0.92. The caregiver’s attitudes toward drug addict’s recovery scale is thus a psychometrically sound tool for the assessment of caregiver’s attitudes toward drug addict’s recovery in Pakistan.
Keywords: attitude, caregivers, drug addicts, Pakistan, recovery, scale development
Main Points
- Caregiver’s attitudes toward recovery of their drug addicted loved one significantly influence adher-ence to treatment and sustainability of sobriety.
- Study aimed to develop and validate a scale for assessment of caregiver’s attitudes toward recovery.
- Caregiver’s attitudes toward drug addict’s recovery scale (CADRS) is a 42-item scale with a four-factor structure explaining 49.01% of total variance
- The CADRS and its subscales (negative recovery expectations, positive recovery expectations, emo-tional resentment, therapeutic pessimism) have a high value of Cronbach’s alpha reliability coef-ficient (≥0.77)
- The convergent and discriminant validity of CADRS was also assessed by using internalized stigma of substance use for caregivers Urdu.
Introduction
Attitudes refer to the individual’s evaluation of an object through the integration of cognitions and affects associated with that object (Crano & Prislin, 2006). McLeod (2018) elaborated attitude in terms of its affective, behavioral, and cognitive components. In the context of drug addicts’ recovery, the literature highlighted caregivers’ feelings of fear, anger, uncertainty, loss, and hopelessness associated with the recovery of their loved one (Horváth & Urban, 2019; Thein et al., 2021). It is also evident that families experience low hope, which might lead to disintegration in seeking opportunities for recovery for their drug addicted loved one (Chen et al., 2022). The qualitative studies (Best et al., 2016; Dekkers et al., 2020) also revealed certain beliefs of caregivers about recovery of their loved one, such as unrealistic expectations from drug addicts and the recovery process; recovery as impossible no matter how much a drug addict or their caregivers try; and the relational process of recovery, where caregivers and drug addicted family members need to have joint efforts toward recovery from drug addiction. The disease model of drug addiction (Jellinek, 1960) also highlighted the belief that drug use is like a disease and recovery is not in the drug addict’s voluntary control. The free-will model of drug addiction, on the contrary, considers it as voluntary behavior characterized by willfulness and responsibility (Schaler, 1991) thus overemphasizing the personality attributes and the individual’s own will for recovery, which also signifies the process of drug addiction treatment. This is because the medical treatment (i.e., detoxification), though improve individual’s drug intake for a brief period but it couldn’t promise lasting effects without the individual’s active participation in the recovery process.
Attitude and behavior are closely associated with each other. The ABC model of attitude elaborates the affective (A), behavioral (B), and cognitive (C) components of attitude. The affective component underlies the feelings or emotions of individuals as associated with the object of attitude. The behavioral component underlies how the attitude shapes and influence the behavior of an individual toward the object of attitude. The third cognitive component of attitude involves an individual’s knowledge, beliefs, and thoughts about the object of attitude. A principle associated with the linkage of attitude and behavior is the principle of consistency, which states that attitude is consistent with behavior (McLeod, 2018). Caregivers of drug addicts are evident from the literature to have feelings of fear, anger, uncertainty, and loss associated with the recovery of their loved one (Thein et al., 2021) which forms the affective component of attitude. The literature also provides information about different beliefs of caregivers about recovery of drug addicts (Best et al., 2016; Dekkers et al., 2020) which forms the cognitive component of attitude. Similarly, caregivers demonstrate varied types of perspectives in seeking the treatment of drug addiction (Andersson et al., 2018; Edwards et al., 2018) i.e., the behavioral component of attitude which might be based on the associated affective and cognitive components.
According to the drug-related locus of control model (Ersche et al., 2012) the attitudes related to recovery from drug addiction closely associate with drug locus of control. It refers to how strongly a drug addict believes they have control over their drug addiction. This belief is significantly associated with the attitude toward drug addiction and steps taken toward getting rid of it; that is, treatment adherence and attitude toward treatment (Murphy & Bentall, 1992). The model explains the locus of control related to drug addiction as the extent of control believed by the drug addicts. The individual might believe that the outcome associated with drug addiction is under their personal control (i.e., internal locus of control) or under the influence of external circumstances (i.e., external locus of control) (Rotter, 1966). It is comprised of two components; that is, locus of control for (a) successful recovery and (b) decisions to use drugs. An internal locus of control, according to this model, will result in an individual’s active involvement in recovery. It also strongly associates with treatment adherence and thus leads to successful recovery from drug addiction. On the contrary, an external locus of control attributes its decision to external circumstances, which reduces the individual’s involvement in the recovery process and thus hinders the successful process of recovery (Ersche et al., 2012).
Different attitudes are thus associated with different behavioral dispositions. Caregivers’ attitudes toward the recovery of their loved one from drug addiction is thus of dire importance to ensure their role in sustained recovery of drug addict. It is also related to the assessment need for caregiver’s attitudes toward recovery. The existing scales for attitudes toward sobriety are not specified to this context. Borkin et al. (2000) for instance developed scale for the assessment of recovery from psychiatric disorders. It is a seven items scale evaluating dimensions of recovery as possible and needs faith, and recovery as difficult, which differs among people. It was found to be psychometrically sound for health professionals, people with mental disorders, family members, and others. Likewise, the sobriety support preference scale (Grant & Dill-Shackleford, 2017) is a 40 items measure assessing the preferences of drug users in seeking sobriety support. It was designed to evaluate beliefs and behaviors associated with face-to-face and online support systems. There is also the availability of scales to assess the attitudes of people toward drug addicts and drug addiction (Bryan et al., 2016; Kalebka et al., 2013; Schaler, 1995) but as per the researcher’s knowledge, there is no scale yet available to assess caregivers’ attitudes toward drug addicts’ recovery. The literature from Pakistan also has a gap in this context. Studies in Pakistan, however, are conducted to assess quality of life (Iqbal & Ijaz, 2024), psychological well-being (Ali & Sadiq, 2011), stigma (Rafiq & Sadiq, 2019), and mental health functioning (Suneel et al., 2020) for the family caregivers of drug addicts. The culturally relevant scale in this regard is also of significance to design family-centered interventions and policy frameworks.
Material Methods
The study followed mixed method cross-sectional study design and was accomplished in three phases such that, phase 1 attempt to generate item pool based on qualitative exploration of the construct on caregivers of drug addicts. Phase 2 determined the factor structure of finalized item pool through exploratory factor analysis (EFA). Phase 3 assessed psychometric properties of developed scale including construct validity through confirmatory factor analysis (CFA), convergent and discriminant validity by comparing scores with internalized stigma of substance use for caregivers (ISSAC-Urdu). The design of the study was approved by the ethical committee (Registration No. 03212111002) at the researcher’s institutional board for advanced studies and research.
Phase 1: Item Pool Generation
The sample of this phase (Table 1) comprised caregivers of drug addicts (N = 17; Mage = 39.35). It was approached through snowball sampling technique. The inclusion criterion for the sample was that caregivers identify themselves as primary caregivers, involved in a caregiving role for at least the last two years, live with drug addicted loved one, there is just one drug addicted loved one to be cared for, and neither the drug addict nor the caregiver has any psychological problem. In-depth interviews were conducted with the help of an interview guideline covering caregivers’ attitudes about the meaning of recovery, ways of recovery, problems during recovery, and the caregiver’s role in the recovery for drug addicted loved one. The interviews were recorded after taking proper informed consent from the participants. They were assured of anonymity and confidentiality of the information. The psychological safety of the caregivers was also considered during interviews; that is, not to ask any questions that might act as a trigger for stress. A debriefing session was conducted after each interview. The data obtained was transcribed and analyzed using interpretative phenomenological analysis from descriptive to interpretative understanding of the data (Azungah, 2018) under a hermeneutic approach; that is, consideration for the sociocultural context of caregivers in drawing the meaning of information they provided (Suddick et al., 2020).
| Table 1. Demographic characteristics for caregivers of drug addicts (N = 17) | |||||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
| M1 |
|
|
|
|
|
|
|
| M2 |
|
|
|
|
|
|
|
| M3 |
|
|
|
|
|
|
|
| Mc1 |
|
|
|
|
|
|
|
| Mc2 |
|
|
|
|
|
|
|
| F1 |
|
|
|
|
|
|
|
| Fc1 |
|
|
|
|
|
|
|
| W1 |
|
|
|
|
|
|
|
| W2 |
|
|
|
|
|
|
|
| Wc1 |
|
|
|
|
|
|
|
| B1 |
|
|
|
|
|
|
|
| B2 |
|
|
|
|
|
|
|
| B3 |
|
|
|
|
|
|
|
| S1 |
|
|
|
|
|
|
|
| S2 |
|
|
|
|
|
|
|
| Sc1 |
|
|
|
|
|
|
|
| So1 |
|
|
|
|
|
|
|
Phase 2: Factor Structure for Developed Scale
Phase 2 of the study attempted to determine the factor structure for the developed scale, that is, caregiver’s attitudes toward drug addict’s recovery scale (CADRS). The objective was accomplished through EFA. Taherdoost et al. (2022) highlighted the significance of EFA for the developed scale because of the limited cultural relevant theoretical basis for the construct. It is essential for identifying the latent constructs underlying a set of observed variables, which helps in defining and representing core dimensions accurately. The majority of items were assessing negative attitudes, so the items assessing positive attitudes toward recovery (1, 2, 4, 5, 6, 9, 14, 15, 16, 37, 38, 39, 40, 41, 42, 43, 44) were reverse coded for the purpose of determining the factor structure. It is also suggested by the literature that reverse coding of items before EFA helps to obtain stable factor structure and avoid factors merely because of item wordings (Fabrigar & Wegener, 2012). The sample comprised 284 caregivers of drug addicts (Table 2) with ages ranging from 23 to 62 years old (Mage= 39.57). The data collection was carried out with the assistance of drug rehabilitation centers in Islamabad, Punjab, Sindh, and Khyber Pakhtunkhwa. All the ethical considerations were taken care of during the stages of data collection, including anonymity, confidentiality, the right to withdraw, and the psychological safety of the participants. The collected data was then analyzed using SPSS 25.
| Table 2. Demographic characteristics of the sample for factor structuring (N = 284) | ||||
|---|---|---|---|---|
| Variables |
|
|
|
|
| Relation with drug addict | Father |
|
|
|
| Mother |
|
|
||
| Wife |
|
|
||
| Brother |
|
|
||
| Sister |
|
|
||
| Son |
|
|
||
| Daughter |
|
|
|
|
| Age | ≤25 years old |
|
|
|
| ≤45 years old |
|
|
||
| ≤65 years old |
|
|
|
|
| Education | ≤10 years of education |
|
|
|
| 10 years of education |
|
|
||
| 12 years of education |
|
|
||
| 14 years of education |
|
|
||
| 16 years of education |
|
|
||
| ≥18 years of education |
|
|
|
|
| Province | Islamabad |
|
|
|
| Punjab |
|
|
||
| Sindh |
|
|
||
| Khyber Pakhtunkhwa |
|
|
|
|
| Duration of loved one’s drug usage | 1–3 years |
|
|
|
| 4–6 years |
|
|
||
| 7–9 years |
|
|
||
| 10–13 years |
|
|
||
| ≥14 years |
|
|
|
|
| Multiple caregivers | Yes |
|
|
|
| No |
|
|
|
|
Phase 3: Psychometric Properties of Developed Scale
The main objective of this phase is to determine the validity and reliability of CADRS. Construct validity was determined through CFA such that the items were hypothesized to possess good indices of model fitness. Convergent and discriminant validity were also determined by comparing scores with ISSA-C Urdu such that scores on subscales of negative recovery expectations, emotional resentment, and therapeutic pessimism would associate positively with scores of internalized stigma, whereas they don’t associate with subscale of positive attitude toward recovery. The ISSA-C Urdu is the Urdu version of ISSA-C (D’Aniello et al., 2022) translated and validated by the researchers of the present study. It assess internalization of stigmatizing attitudes toward adults with drug addiction signified by alienation, stereotype endorsement, perceived discrimination, social withdrawal, and stigma resistance. The scale comprised of 29 items rated on a four-point Likert type scale such that 1 denotes strongly disagree, 2 denotes disagree, 3 denotes agree, and 4 denotes strongly agree. The total range of scores on the scale is from 1 to 116. Items 7, 14, 24, 26, and 27 of the scale are reverse coded. A sample of 400 caregivers of drug addicts (Mage= 43.38) was approached through snowball sampling technique with the assistance of drug rehabilitation centers in Islamabad, Punjab, Sindh, and Khyber Pakhtunkhwa. It comprised of parents, spouses, siblings, and children of drug addicts who were above 20 years old, lived with a drug addict, and had no history of any psychological problem (Table 3). All ethical considerations were taken care of during data collection from caregivers.
| Table 3. Demographic characteristics of the sample for construct validity and psychometric properties (N = 400) | ||||
|---|---|---|---|---|
| Variables |
|
|
|
|
| Relation with drug addict | Father |
|
|
|
| Mother |
|
|
||
| Wife |
|
|
||
| Brother |
|
|
||
| Sister |
|
|
||
| Son |
|
|
||
| Daughter |
|
|
|
|
| Age | ≤25 years old |
|
|
|
| ≤45 years old |
|
|
||
| ≤65 years old |
|
|
|
|
| Education | ≤10 years of education | |||
| 10 years of education | ||||
| 12 years of education | ||||
| 14 years of education | ||||
| 16 years of education | ||||
| ≥18 years of education | ||||
| Province | Islamabad |
|
|
|
| Punjab |
|
|
||
| Sindh |
|
|
||
| Khyber Pakhtunkhwa |
|
|
|
|
| Duration of loved one’s drug usage | 1–3 years |
|
|
|
| 4–6 years |
|
|
||
| 7–9 years |
|
|
||
| 10–13 years |
|
|
||
| ≥14 years |
|
|
|
|
| Multiple caregivers | Yes |
|
|
|
| No |
|
|
|
|
Results
Phase 1: Item Pool Generation
The information obtained from caregivers resulted in three major themes for caregiver’s attitudes toward drug addict’s recovery (Table 4) that are, beliefs (relapse as inevitable, internal-external locus of control for recovery), negative feelings (hopelessness, fear of relapse, frustration, distrust on drug addict, helplessness, distrust on rehabilitation center), and active involvement (access treatment, monitor loved one’s activities, compassion toward loved one, engage loved one in healthy activities, provide religious/spiritual guidance) associated with the recovery of drug addicted loved one. This information was used to initially generate an item pool of 72 statements (29 for positive attitudes and 43 for negative attitudes). All the initial items were critically reviewed by the researcher and supervisor to address any issues with comprehension, redundancy, complexity, ambiguity, and cultural relevance. The response format of a five-point Likert type was also decided at this stage such that 1 denotes Completely False, 2 denotes False, 3 denotes Don’t Know, 4 denotes Completely True, and 5 denotes True. Likert type scales may meet the research needs when researchers are interested in measuring attitude, belief, or behavior items as they improve understanding and thus increase response rate and response quality (Krosnick et al., 2018).
| Table 4. Superordinate and subordinate themes of data obtained from Caregivers (N = 17) | |||
| Superordinate Themes | Subordinate Themes | Description | Relevant Existing Literature |
| Beliefs about recovery | Relapse in inevitable | Relapse to drug use always occur after a period of sobriety. “Once someone gets involved in drug use, there’s no way stopping them. Family members’ attempts to dissuade them are of no use. The person keeps suffering their whole life, and it doesn’t make any difference to them.” (Fc1) | Edwards et al., 2018 |
| Internal locus of control | Recovery from drug addiction is in the drug addict’s own control thus signified individual involvement. “Drug addiction is not a disease as once treated for a disease you know that the person has now recovered. But it couldn’t be like that for an addict until he is willing for sobriety and use his willpower to control the drug addiction.” (B1) | No literature support was found | |
| External locus of control | Recovery from drug addiction is in the control of external circumstances like: | ||
| Biological factors, “My brother tries a lot to quit drug addiction on his own, but he isn’t able to do it. Obviously, addiction changes a person’s brain so it isn’t in their control to stop using drugs and never have them again.” (S1) | (VanDerNagel et al., 2018) | ||
| Early age of onset, “The individuals who start drug use later in life are mature and might be able to control it and recover. But the one who start using drugs at a younger age might not give up drug use ever.” (W1) | (Meulewaeter et al., 2022) | ||
| Peer influence, “When the person is young, he think drug use as a fashion symbol. If he have drugs, the friends will appraise and approve him.” (B1) | (Karakos, 2014) | ||
| Opportunity to use drugs, “…obviously, when you get a room to practice what you wish too, then you practice it. Once a drug addict thus will stay drug addict forever.” (W1) | (Strickland & Smith, 2014) | ||
| Absence of strict action by government against drugs, “There are drug dens everywhere and obviously everyone knows but nobody does anything to control it. Why don’t the law enforcement agencies of the government take any action against these drug dens?” (B1) | (Rasheed et al., 2019; Yaqub, 2013) | ||
| Lack of affordable treatment, “Rehabilitation centers ask for a lot of money which is problematic. If there would be a treatment center of government and treat addict for affordable payment, it will be a lot easier for us. We could have then be able to treat our son for at least six months or a year.” (F1) | (Lister et al., 2020; Thein et al., 2021) | ||
| Absence of compassion by health professionals, “I got my son treated from a government institute. They have a very non caring attitude. I also launch a complaint to higher authorities but they responded back stating that it isn’t their responsibility.” (M3) | (Monks et al., 2013) | ||
| Inappropriate treatment procedures, “The center where we last got my husband treated from used some medicines of which he had strong cravings. Then, only a month later, he started using drugs again.” (W2) | No literature support was found | ||
| Societal stigma, “It takes a lot of effort to get rid of addiction and even after that, if people keep on calling the person drug addict, then obviously he returns to drug use.” (B2) | (Wogen & Restrepo, 2020) | ||
| Negative feelings about recovery | Hopelessness | Feeling that recovery from drug addiction is impossible. “Whenever we admit our dad for treatment, he runs away from there. So, what can we do now? There is probably no solution except that he is tied up and kept in hospital forever which obviously is not possible.” (So1) | (Nodar, 2012; Thein et al., 2021) |
| Fear of relapse | Feeling afraid that the drug addicted loved one will start using the drugs soon after the treatment. “I don’t know about the thoughts of other family members at that time, but I used to think a lot about what if God forbids, he starts using drugs again after treatment.” (B3) | (Kelly et al., 2018) | |
| Frustration | Feeling high emotional tiredness and fed up of trying to seek recovery for drug addicted loved one. “There’s no place left for us to live with dignity. I can’t tolerate this anymore. I wish someone should take him away for treatment and keep him there forever or if a car hits him to death, let it be—just get him out of our lives.” (Fc1) | (Shishkova & Bocharov, 2022) | |
| Distrust on drug addict | Feeling high distrust on loved one for seeking recovery from drug addiction. “We knew he would be using drugs again within 24hrs after treatment…he just can’t leave them.” (B1) | No literature support was found | |
| Helplessness | Caregivers express helplessness about controlling drug use and any further efforts seems meaningless. “How long I and my husband need to keep caretaking him? We’ve made so many efforts, but now it just feels like it would be useless to try anymore.” (Sc1) | (Settley, 2020; Mikulic et al., 2023) | |
| Distrust on rehabilitation center | Caregivers mentioned about lacking trust on rehabilitation centers for loved one recovery. “I don’t know how they treat our children or what they do with them. In the previous institution where I admitted my child, he was lying unconscious. This institution seems better, but I still am a lot scared and worried about my child’s safety here.” (Mc2) | No literature support was found | |
| Active involvement for recovery | Access treatment | Avail the treatment opportunities for the drug addicted loved one. “Rehabilitation centers make a perfect routine and all things are properly scheduled. So, treatment is the only best solution for leaving drugs and live a sober life.” (B1) | (Cornelius et al., 2017; Edwards et al., 2018; Earnshaw et al., 2019) |
| Monitor loved one’s activities | Monitor the activities of loved one to assure their abstinence from drug use. “Obviously, he finds comfort in drugs and we can’t monitor him so he kept on using drugs. There must be a proper person hired just to stay with him, take care of him, and keep constant check over him.” (S1) | (Dekkers et al., 2020; Masood & Sahar, 2014) | |
| Compassion toward loved one | Stay kind and caring toward the drug addicted loved one to help them recovery from addiction. “The journey of getting rid of drugs is extremely difficult and painful for a drug addict. At this point, he needs the support and care from his family and friends.” (B3) | (Bartlett et al., 2013) | |
| Engage loved one in healthy activities | Engaged the drug addicted loved one in daily healthy activities to sustain their sobriety. “If we keep a person busy in any type of work then his mind does not go towards thoughts of drug addiction.” (W2) | (Davidson et al., 2010; Snoek et al., 2016) | |
| Provide religious/ spiritual guidance | Religious/spiritual guidance to drug addicted loved one about harms and consequences of drug use. “Getting rid of drug addiction can be done only if the person realizes that it is ruining his life and relations. In this regard, only God can guide a person, otherwise it is very difficult.” (B1) | (Charzynska, 2021; Weinandy & Grubbs, 2021) | |
The refined item pool (44 items) was then further reviewed by subject matter experts (SMEs) to establish content validity. The experts included two assistant professors and three PhD scholars of Psychology who have experience in scale development. For five experts, the recommended content validity ratio (CVR) for each item is 1.00 (Ayre & Scally, 2014; Lawshe, 1975). All 44 items were considered essential for the assessment of the construct. Item 35 was, however, considered poorly structured by one expert and thus rephrased. The CVR for the items is thus greater than 1.00, and thus all 44 items were retained for the final version. The statements reflected both positive and negative caregivers’ attitudes toward drug addicts, such as, “I believe my loved one will quit drugs if they are made to feel responsible” (item 6) and “The accessibility of drugs abstain my loved one to recover from drug use.” (item 8)
Phase 2: Factor Structure for Developed Scale
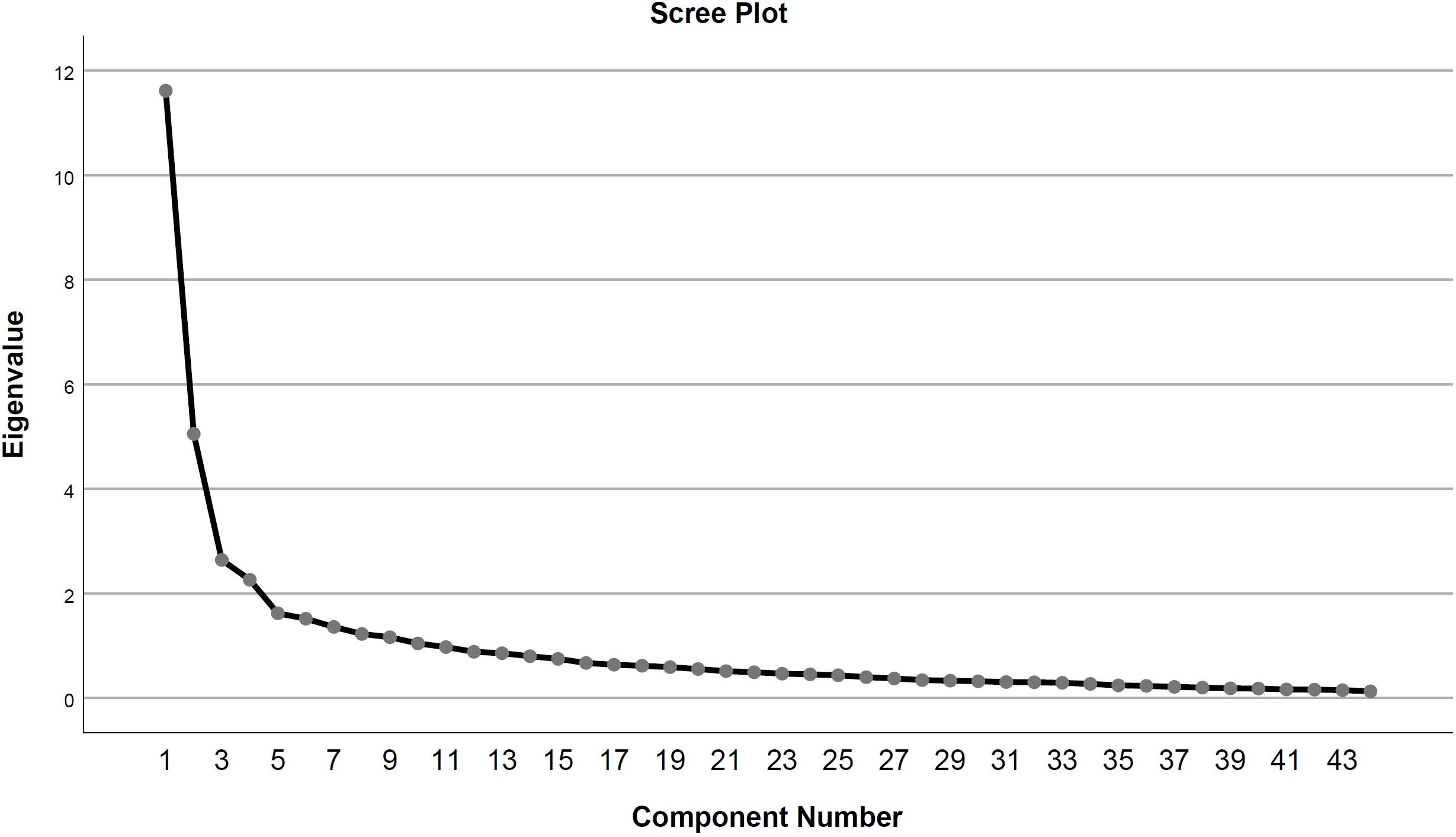
The factorial structure of caregiver’s attitudes toward drug addict’s Recovery Scale was examined with the help of EFA technique. Bartlett’s test of sphericity was significant (χ2 (946) = 7131.60, p < 0,001), which demonstrates that the items possess adequate common variance for the conduction of factor analysis; that is, items could lead to the definite factor structures by the EFA. Kaiser-Meyer-Olkin Measure of sample adequacy was 0.87, which is close to 1, thus suggesting that the data set is adequate for the factor structuring (Field, 2024). The findings from both of these measures support the decision of factor analysis for the scale. The inter-item correlations generated by EFA demonstrate that the items are not highly correlated (i.e., >0.07), which provides rationale for using an orthogonal type of rotation such as varimax rotation (Osborne, 2015). The scree plot (Figure 1) demonstrate four-factor solution such that factor 1 explains 18.56% variance, factor 2 explains 16.36%, factor 3 explains 7.56%, and factor 4 explains 6.53% of the total variance in caregiver’s attitudes toward drug addict’s recovery. All the 44 items contribute to 49.01% of the total variance (Table 5) with good factor loadings (> 0.30). The factor loadings of items under respective factors are highlighted in bold. The factor naming was done with the help of three SMEs who were PhD scholars with experience in scale development. The subscales were thus labeled as negative recovery expectations (3, 7, 8, 10, 11, 12, 13, 20, 21, 23, 28, 30, 31, 32, 33, 34, 35, 36), positive recovery expectations (1, 2, 5, 6, 9, 14, 15, 16, 37, 38, 39, 40, 41, 42, 43, 44), emotional resentment (4, 24, 25, 26, 27, 29), and therapeutic pessimism (17, 18, 19, 22). “I fear my loved one won’t quit drugs even after treatment” (item 3) reflects negative recovery expectations, “I believe that with my persistent efforts, my loved one will abstain from drug use” (item 14) reflects positive recovery expectations, “I feel that I have to make lifelong efforts for recovery of my loved one from drug addiction” (item 25) reflects emotional resentment, and “I believe spending money on my loved one’s treatment is a waste” (item 17) reflects therapeutic pessimism.
| Table 5. Factor loadings and communalities for caregiver’s attitudes toward drug addict’s recovery scale (N = 284) | |||||
| Factor Loadings | |||||
| Items |
|
|
|
|
|
| 33. |
|
|
|
||
| 8. |
|
|
|
|
|
| 7. |
|
|
|
||
| 10. |
|
|
|||
| 32. |
|
|
|
|
|
| 31. |
|
|
|
|
|
| 20. |
|
|
|
|
|
| 12. |
|
|
|
|
|
| 21. |
|
|
|
|
|
| 30. |
|
|
|
|
|
| 35. |
|
|
|
|
|
| 11. |
|
|
|
|
|
| 36. |
|
|
|
||
| 34. |
|
|
|
|
|
| 13. |
|
|
|
|
|
| 28. |
|
|
|
|
|
| 23. |
|
|
|
|
|
| 3. |
|
|
|
|
|
| 2. |
|
|
|
||
| 14. |
|
|
|
||
| 15. |
|
|
|
||
| 6. |
|
|
|||
| 38. |
|
|
|
||
| 40. |
|
|
|
|
|
| 1. |
|
|
|
|
|
| 39. |
|
|
|
|
|
| 41. |
|
|
|
||
| 43. |
|
|
|
|
|
| 37. |
|
|
|
|
|
| 9. |
|
|
|
|
|
| 16. |
|
|
|
|
|
| 44. |
|
|
|
|
|
| 42. |
|
|
|
|
|
| 5. |
|
|
|
|
|
| 26. |
|
|
|
|
|
| 27. |
|
|
|
|
|
| 25. |
|
|
|
|
|
| 29. |
|
|
|
|
|
| 24. |
|
|
|
|
|
| 4. |
|
|
|
|
|
| 18. |
|
|
|
|
|
| 17. |
|
|
|
|
|
| 22. |
|
|
|
|
|
| 19. |
|
|
|
|
|
| Eigen values |
|
|
|
||
| Percentage of variance explained |
|
|
|
||
| Cumulative percentage |
|
|
|||
Phase 3: Psychometric Properties of Developed Scale
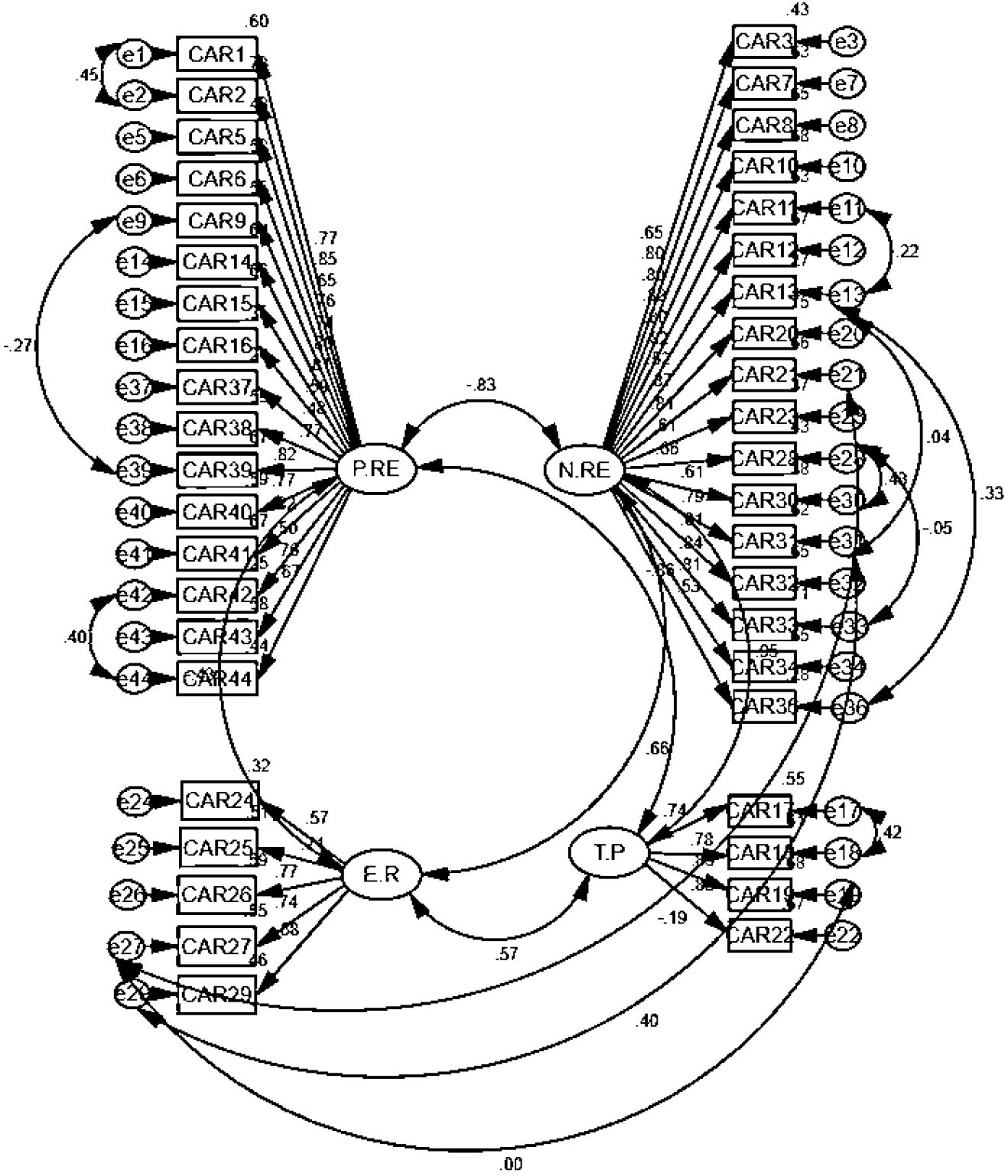
The construct validity of the factor structure determined in phase 2 was used to assess model fitness using CFA. The results demonstrate good factor loadings for 42 out of the 44 items (>0.40) showing significant contribution in explaining the construct (Table 6). “I firmly believe that my loved one can quit drug use if they want to” (item 4) and “I believe I need to find a better treatment for my loved one” (item 35) were removed due to poor factor loadings (<0.25). The model fit indices (Table 7) demonstrated that the improvement of model fit from model 1 to model 2 was achieved by the application of error covariances applied between the error terms (Figure 2). This helped to decrease the error variance and hence led to the model fit (Divers et al., 2011; Kim & Kim, 2018). Alpha coefficients show good reliabilities for subscales: negative recovery expectations (α = 0.92), positive recovery expectations (α = 0.89), emotional resentment (α = 0.77), and therapeutic pessimism (α = 0.79). Convergent validity was also assessed through correlation estimates. It demonstrates that, as hypothesized internalized stigma is significantly correlated with negative recovery expectations (r = 0.24, p = 0.001), emotional resentment (r = 0.42, p = 0.000), and therapeutic pessimism (r = 0.25, p = .001). Internalized stigma however don’t associate with positive attitude toward recovery (r = −0.11, p = 0.14), such that items of this subscale were not reverse-coded for the purpose of determining the discriminant validity of the subscale with ISSA-C Urdu.
| Table 6. Factor loadings (standardized regression weights) for caregiver’s attitudes toward drug addict’s recovery scale (42-ıtems) (n = 400) | |||||||
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
||||||
| Table 7. Confirmatory factor analysis of caregiver’s attitudes toward drug addict’s recovery scale (ındices of model fit) (n = 400) | |||||||||
| Model |
|
|
|
|
|
||||
|
|
|
|
|
|
|||||
| Model-1 first order CFA (44 items—without error covariances) | |||||||||
|
|
|
|
|
|
|
|
|
|
|
| Model-2 first order CFA (42 items—with error covariances) | |||||||||
|
|
|
|
|
|
|
|
|
|
|
Discussion
The study is accomplished in three phases such that phase 1 attempted to generate an item pool based on the information from in-depth interviews with caregivers. The caregivers’ attitudes toward drug addicts’ recovery were found to be comprised of beliefs, negative feelings, and active involvement in the recovery of drug addicts. The indigenous perspective revealed beliefs of internal locus of control for recovery (active involvement and willingness of drug addicts) and inappropriate treatment procedures for recovery, feelings of distrust on drug addict and rehabilitation centers for efforts of sustained sobriety. The refined item pool consisted of 44 items with good content validity as determined by CVR. The factor structure in phase 2 results in a four-factor solution for the developed scale explaining 49.01% of total variance, such that a high score on the subscale of negative recovery expectations (18 items) demonstrates caregivers’ hopelessness, pessimism, and perceived barriers to the recovery of their loved ones. The high score on the subscale of positive recovery expectations (16 items) demonstrates caregivers’ hope, trust, and belief in recovery through support and treatment. Similarly, a high score on emotional resentment (6 items) indicates feelings of being tired, irritated, frustrated, and on the verge of giving up the efforts to seek recovery for drug addicted loved ones. Likewise, the high score on the subscale of therapeutic pessimism (4 items) demonstrates hopelessness and skepticism about the worth of treatment seeking for recovery. Both of the aforementioned subscales closely associate with subscale of negative recovery expectations but appear as an independent factors for the construct. The factor loadings and communalities (i.e., unique variance) were found to be high for all the items which demonstrates reliable and valid nature of the scale (Gaskin & Happell, 2014).
Phase 3 of the study carried out the construct validity of CADRS. The factor loadings for 42 out of 44 items were good (>0.50) (Table 6). The item 4, “I firmly believe that my loved one can quit drug use if they want to” and item 35, “I believe I need to find a better treatment for my loved one” were removed due to poor factor loadings (<0.25). Literature also demonstrates that items with low factor loadings need to be considered for removal as they depict poor representation of the construct (Hair et al., 2010). Item 4 measures belief in trust on loved one about willingness to abstain from drug use. The reason for poor factor loading could be that another item of the scale assesses the same concept and is more comprehensible, “I firmly believe that my loved one could quit drug use forever” (item 1). It is also evident from literature that items which are difficult to comprehend by the sample might have a poor contribution to the construct (DeVellis, 2017). The content of item 35, on the other hand, appears to be assessing attitude toward treatment for recovery more specifically than attitude toward recovery, which might be the reason for poor factor loading.
Goodness fit of the model based on 42 retained items for CADRS was achieved by drawing error covariances between the items (Table 7) which results in decreasing the error variance and hence improving overall fitness of the model (Kim & Kim, 2018). It was observed that the error covariances were drawn between the items of different factors (Figure 2) which is indicative that these factors possess a statistically significant relation to one another. The content of the items also provides additional support for the similarity. Error covariance was added between item 1 “I firmly believe that my loved one could quit drug use forever” and reverse coded item 27 “I get very angry with my drug using loved one.” These two statements are associated as when caregiver trusts the loved one for quitting drugs they don’t feel angry with them. It is also evident from literature that distrust is associated with feelings of anger (Wallace, 2019). Likewise, there was an error covariance between item 16 “I believe that in the company of good friends, my loved one will quit using drugs” showing importance of good company for abstaining from drugs and the reverse coded item 24 “I feel that drug use is more important to my loved one than my love and sincerity” indicating consideration of caregiver’s loving attitude over drug use. Literature also supports the association between these two statements as good company (Tracy & Wallace, 2016) and caregiver’s compassion (Bartlett et al., 2013) could provide help in moving toward a sober lifestyle.
Error variance for reverse coded item 9 “I believe that if my loved one/relative does not have the opportunity to use drugs, he will quit” relates to that of item 36 “I feel that I cannot help my loved one to quit drugs because the treatment is expensive” and reverse coded item 39 “I understand that my loved one needs my trust to stop using drugs.” Reverse coding items 9 and 39 shows an absence of hope for recovery even in the absence of opportunity for drug use and trust of the caregiver, respectively. This negative attitude might be associated with similar behavior toward recovery as not being able to seek treatment considering it expensive (item 36). Similarly, a covariance is also added for item 17 “I think that getting treatment for my loved one is just a waste of money” and reverse coded item 14 “I believe that my loved one will stop using drugs with my persistent efforts.” Reverse coded item 14 shows the caregiver’s hopelessness that a loved one can’t leave drug use no matter how much effort is made, which associates with a negative perspective about treatment for recovery (item 17). Researchers also support that the hopelessness of caregivers might result in restricting efforts toward recovery (Thein et al., 2021).
The error variance for item 29 “I feel like I can’t keep an eye on my loved one all the time to get rid of drug use” relates to that of item 30 “I feel that my loved one doesn’t want to stop using drugs” and item 31 “I feel that my loved one makes no effort to stop using drugs.” Items 30 and 31 demonstrate distrust of the loved one to quit drug use, which relates to the negative attitude of making an effort toward their recovery by constant monitoring (item 29). Distrust by caregivers might affect the efforts to seek recovery; however, literature support for this relation was not found. Error variance for reverse coded item 37 “I am sure that if my loved one is being watched all the time, he will stop using drugs” relates to that of item 25 “I feel that I have to struggle my whole life to get my loved one to quit using drugs” and item 28 “I feel that the drug-using loved one isn’t concerned about my worries.” Reverse coding item 37 reflects the caregiver’s belief that the loved one can’t leave drugs even when being watched, which associates with exhaustion in seeking recovery (item 25) and frustration toward the loved one for being unconcerned about the caregiver’s worry (item 28). Literature also supports that negative belief or perspective about recovery is associated with exhaustion and frustration (Shishkova & Bocharov, 2022) among caregivers of drug addicts.
The results also demonstrate that the reliabilities for all subscales were high (>0.70) which indicate internal consistency of scores (Hajjar, 2018; Kalkbrenner, 2021). Convergent validity for CADRS was also assessed through high correlation with scores on psychometrically valid instrument(s) assessing the same or similar construct. Likewise, there was an absence of correlation with scores on psychometrically valid instrument(s) assessing a different construct, respectively. Researchers highlight the significance of convergent and discriminant validity in scale development to support its psychometric soundness (Campbell & Fiske, 1959; DeVellis, 2017). In the present study ISSA-C Urdu assessing internalized stigma for caregivers was used to determine convergent and discriminant validity. It is also evident from the literature that a high degree of internalized stigma among caregivers of drug addicts is associated with considering recovery from drug addiction as impossible and stop seeking recovery for drug addict (Corrigan et al., 2019) that is, a negative attitude toward recovery. The results demonstrated that, as hypothesized internalized stigma is significantly correlated with negative attitude toward recovery and feelings of exhaustion during recovery. It is, however, not correlated with a positive attitude toward recovery.
Limitations and Suggestions for Future Research
The major limitation of the present study is that caregivers of only male drug addicts were included as per the convenience of data collection. Future studies may include those of female drug addicts to determine more generalizable psychometric properties of developed scale. Another limitation is the inclusion of only one scale for assessing convergent and discriminant validity of the developed scale. Future researchers could support findings by using some other scales for comparison.
Ethical approval
This study was approved by the Ethics Committee of Quaid-i-Azam University, Islamabad (Date: February 23, 2021, Decision/Protocol No: 03212111002). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Ali, A. Z., & Sadiq, R. (2011). Psychological problems in wives of adults with substance abuse problem. Pakistan Journal of Clinical Psychology, 10(2). https://pjcpku.com/index.php/pjcp/article/view/114
- Andersson, C., Best, D., Irving, J., Edwards, M., Banks, J., Mama-Rudd, A., & Hamer, R. (2018). Understanding recovery from a family perspective: A survey of life in recovery for families. Sheffield Hallam University for Alcohol Research UK.
- Ayre, C., & Scally, A. J. (2014). Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), 79-86. https://doi.org/10.1177/0748175613513808
- Azungah, T. (2018). Qualitative research: Deductive and inductive approaches to data analysis. Qualitative Research Journal, 18(4), 383-400. https://doi.org/10.1108/QRJ-D-18-00035
- Bartlett, R., Brown, L., Shattell, M., Wright, T., & Lewallen, L. (2013). Harm reduction: Compassionate care of persons with addictions. Medsurg Nursing: Official Journal of the Academy of Medical-Surgical Nurses, 22(6), 349.
- Best, D., Beckwith, M., Haslam, C., Alexander Haslam, S., Jetten, J., Mawson, E., & Lubman, D. I. (2016). Overcoming alcohol and other drug addiction as a process of social identity transition: The social identity model of recovery (SIMOR). Addiction Research and Theory, 24(2), 111-123. https://doi.org/10.3109/16066359.2015.1075980
- Borkin, J. R., Steffen, J. J., Ensfield, L. B., Krzton, K., Wishnick, H., Wilder, K., & Yangarber, N. (2000). Recovery Attitudes Questionnaire: Development and evaluation. Psychiatric Rehabilitation Journal, 24(2), 95-102. https://doi.org/10.1037/h0095112
- Bryan, C. J., Yeager, D. S., Hinojosa, C. P., Chabot, A., Bergen, H., Kawamura, M., & Steubing, F. (2016). Harnessing adolescent values to motivate healthier eating. Proceedings of the National Academy of Sciences of the United States of America, 113(39), 10830-10835. https://doi.org/10.1073/pnas.1604586113
- Campbell, D. T., & Fiske, D. W. (1959). Convergent and discriminant validation by the multitrait-multimethod matrix. Psychological Bulletin, 56(2), 81-105. https://doi.org/10.1037/h0046016
- Charzyńska, E. (2021). The effect of baseline patterns of spiritual coping, forgiveness, and gratitude on the completion of an alcohol addiction treatment program. Journal of Religion and Health, 60(3), 1796-1817. https://doi.org/10.1007/s10943-021-01188-8
- Chen, A. T., Johnny, S., & Conway, M. (2022). Examining stigma relating to substance use and contextual factors in social media discussions. Drug and Alcohol Dependence Reports, 3, 100061. https://doi.org/10.1016/j.dadr.2022.100061
- Cornelius, T., Earnshaw, V. A., Menino, D., Bogart, L. M., & Levy, S. (2017). Treatment motivation among caregivers and adolescents with substance use disorders. Journal of Substance Abuse Treatment, 75, 10-16. https://doi.org/10.1016/j.jsat.2017.01.003
- Corrigan, P. W., Qin, S., Davidson, L., Schomerus, G., Shuman, V., & Smelson, D. (2019). How does the public understand recovery from severe mental illness versus substance use disorder?. Psychiatric Rehabilitation Journal, 42(4), 341-349. https://doi.org/10.1037/prj0000380
- Crano, W. D., & Prislin, R. (2006). Attitudes and persuasion. Annual Review of Psychology, 57, 345-374. https://doi.org/10.1146/annurev.psych.57.102904.190034
- D’Aniello, C., Tambling, R., & Russell, B. (2022). The internalized stigma of substance abuse scale for caregivers: Measuring substance use stigma experienced by caregivers. Alcoholism Treatment Quarterly, 40(1), 83-92. https://doi.org/10.1080/07347324.2021.1941473
- Davidson, L., White, W., Sells, D., Schmutte, T., O'Connell, M., Bellamy, C., & Rowe, M. (2010). Enabling or engaging? The role of recovery support services in addiction recovery. Alcoholism Treatment Quarterly, 28(4), 391-416. https://doi.org/10.1080/07347324.2010.511057
- Dekkers, A., De Ruysscher, C., & Vanderplasschen, W. (2020). Perspectives on addiction recovery: Focus groups with individuals in recovery and family members. Addiction Research and Theory, 28(6), 526-536. https://doi.org/10.1080/16066359.2020.1714037
- DeVellis, R. F. (2017). Scale development: Theory and applications (4th ed., pp. 123). Sage Publications.
- Divers, J., Redden, D. T., Carroll, R. J., & Allison, D. B. (2011). How to estimate the measurement error variance associated with ancestry proportion estimates. Statistics and Its Interface, 4(3), 327-337. https://doi.org/10.4310/SII.2011.v4.n3.a7
- Earnshaw, V. A., Bogart, L. M., Menino, D. D., Kelly, J. F., Chaudoir, S. R., Reed, N. M., & Levy, S. (2019). Disclosure, stigma, and social support among young people receiving treatment for substance use disorders and their caregivers: A qualitative analysis. International Journal of Mental Health and Addiction, 17(6), 1535-1549. https://doi.org/10.1007/s11469-018-9930-8
- Edwards, M., Best, D., Irving, J., & Andersson, C. (2018). Life in recovery: A families’ perspective. Alcoholism Treatment Quarterly, 36(4), 437-458. https://doi.org/10.1080/07347324.2018.1488553
- Ersche, K. D., Turton, A. J., Croudace, T., & Štochl, J. (2012). Who do you think is in control in addiction? A pilot study on drug-related locus of control beliefs. Addictive Disorders and Their Treatment, 11(4), 173-223. https://doi.org/10.1097/ADT.0b013e31823da151
- Fabrigar, L. R., & Wegener, D. T. (2012). Exploratory factor analysis. Oxford University Press.
- Field, A. (2024). Discovering statistics using IBM SPSS Statistics. Sage Publications.
- Gaskin, C. J., & Happell, B. (2014). On exploratory factor analysis: A review of recent evidence, an assessment of current practice, and recommendations for future use. International Journal of Nursing Studies, 51(3), 511-521. https://doi.org/10.1016/j.ijnurstu.2013.10.005
- Grant, D. S., & Dill-Shackleford, K. E. (2017). Using social media for sobriety recovery: Beliefs, behaviors, and surprises from users of face-to-face and social media sobriety support. Psychology of Popular Media Culture, 6(1), 2-20. https://doi.org/10.1037/ppm0000126
- Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis: A global perspective (7th ed., pp. 137). Pearson Education.
- Hajjar, S. T. (2018). Statistical analysis: Internal-consistency reliability and construct validity. International Journal of Quantitative and Qualitative Research Methods, 6(1), 27-38.
- Horváth, Z., & Urbán, R. (2019). Testing the stress-strain-coping-support (SSCS) model among family members of an alcohol misusing relative: The mediating effect of burden and tolerant-inactive coping. Addictive Behaviors, 89, 200-205. https://doi.org/10.1016/j.addbeh.2018.10.010
- Iqbal, M. N., & Ijaz, S. (2024). Exploring psychosocial determinants of quality of life in young adults with paternal substance use disorder in Pakistan: A phenomenological study. Journal of Substance Use, 1-6. https://doi.org/10.1080/14659891.2024.2322154
- Jellinek, E. M. (1960). The disease concept of alcoholism. Hillhouse Press. https://doi.org/10.1037/14090-000
- Kalebka, R. R., Bruijns, S. R., & Van Hoving, D. J. (2013). A survey of attitudes towards patient substance abuse and addiction in the Emergency Centre. African Journal of Emergency Medicine, 3(1), 10-17. https://doi.org/10.1016/j.afjem.2012.09.004
- Kalkbrenner, M. T. (2021). Alpha, omega, and H internal consistency reliability estimates: Reviewing these options and when to use them. Counseling Outcome Research and Evaluation, 14(1), 77-88. https://doi.org/10.1080/21501378.2021.1940118
- Karakos, H. L. (2014). Positive peer support or negative peer influence? The role of peers among adolescents in recovery high schools. Peabody Journal of Education, 89(2), 214-228. https://doi.org/10.1080/0161956X.2014.897094
- Kelly, J. F., Greene, M. C., & Bergman, B. G. (2018). Beyond abstinence: Changes in indices of quality of life with time in recovery in a nationally representative sample of US adults. Alcoholism: Clinical and Experimental Research, 42(4), 770-780. https://doi.org/10.1111/acer.13604
- Kim, S. M., & Kim, H. M. (2018). Effect of observation error variance adjustment on numerical weather prediction using forecast sensitivity to error covariance parameters. Tellus A: Dynamic Meteorology and Oceanography, 70(1), 1-16. https://doi.org/10.1080/16000870.2018.1492839
- Krosnick, J. A., Judd, C. M., & Wittenbrink, B. (2018). The measurement of attitudes. In The handbook of attitudes, 1: Basic Principles (pp. 45-105). Routledge.
- Lawshe, C. H. (1975). A quantitative approach to content validity. Personnel Psychology, 28(4), 563-575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x
- Lister, J. J., Weaver, A., Ellis, J. D., Himle, J. A., & Ledgerwood, D. M. (2020). A systematic review of rural-specific barriers to medication treatment for opioid use disorder in the United States. The American Journal of Drug and Alcohol Abuse, 46(3), 273-288. https://doi.org/10.1080/00952990.2019.1694536
- Masood, S., & Us Sahar, N. (2014). An exploratory research on the role of family in youth's drug addiction. Health Psychology and Behavioral Medicine: An Open Access Journal, 2(1), 820-832. https://doi.org/10.1080/21642850.2014.939088
- McLeod, S. A. (2018). Attitudes and behavior. https://www.simplypsychology.org/attitudes.htm
- Meulewaeter, F., De Schauwer, E., De Pauw, S. S., & Vanderplasschen, W. (2022). “I grew up amidst alcohol and drugs:” A qualitative study on the lived experiences of parental substance use among adults who developed substance use disorders themselves. Frontiers in Psychiatry, 13, 768802. https://doi.org/10.3389/fpsyt.2022.768802
- Mikulić, M., Ćavar, I., Jurišić, D., Jelinčić, I., & Degmečić, D. (2023). Burden and Psychological Distress in Caregivers of Persons with Addictions. Challenges, 14(2), 24. https://doi.org/10.3390/challe14020024
- Monks, R., Topping, A., & Newell, R. (2013). The dissonant care management of illicit drug users in medical wards, the views of nurses and patients: A grounded theory study. Journal of Advanced Nursing, 69(4), 935-946. https://doi.org/10.1111/j.1365-2648.2012.06088.x
- Murphy, P. N., & Bentall, R. P. (1992). Motivation to withdraw from heroin: A factor-analytic study. British Journal of Addiction, 87(2), 245-250. https://doi.org/10.1111/j.1360-0443.1992.tb02698.x
- Nodar, M. (2012). Chaotic environments and adult children of alcoholics. The Professional Counselor: Research and Practice, 2(1), 43-47. https://doi.org/10.15241/mnn.2.1.43
- Osborne, J. W. (2015). What is rotating in exploratory factor analysis? Practical Assessment, Research, and Evaluation, 20(1), 2. https://doi.org/10.7275/hb2g-m060
- Rafiq, M., & Sadiq, R. (2019). Caregiver stress, perceived stigma and mental health in female family members of substance users: Correlational Study. JPMA. the Journal of the Pakistan Medical Association, 69(9), 1300-1303.
- Rasheed, H., Hoellein, L., Bukhari, K. S., & Holzgrabe, U. (2019). Regulatory framework in Pakistan: Situation analysis of medicine quality and future recommendations. Journal of Pharmaceutical Policy and Practice, 12(1), 1- 15 https://doi.org/10.1186/s40545-019-0184-z
- Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80(1), 1-28. https://doi.org/10.1037/h0092976
- Schaler, J. A. (1991). Drugs and free will. Society, 28(6), 42-49. https://doi.org/10.1007/BF02695758
- Schaler, J. A. (1995). The addiction belief scale. International Journal of the Addictions, 30(2), 117-134. https://doi.org/10.3109/10826089509060737
- Settley, C. (2020). The physical and psychological wellbeing of caregivers of individuals suffering from substance addiction. Archives of Psychiatric Nursing, 34(3), 107-109. https://doi.org/10.1016/j.apnu.2020.03.007
- Shishkova, A. M., & Bocharov, V. V. (2022). The burnout concept as a theoretical framework for investigating the caregiving impact of relatives of patients with addictive disorders. Psychology in Russia: State of the Art, 15(3), 111-132. https://doi.org/10.11621/pir.2022.0307
- Snoek, A., Levy, N., & Kennett, J. (2016). Strong-willed but not successful: The importance of strategies in recovery from addiction. Addictive Behaviors Reports, 4, 102-107. https://doi.org/10.1016/j.abrep.2016.09.002
- Strickland, J. C., & Smith, M. A. (2014). The effects of social contact on drug use: behavioral mechanisms controlling drug intake. Experimental and Clinical Psychopharmacology, 22(1), 23.
- Suddick, K. M., Cross, V., Vuoskoski, P., Galvin, K. T., & Stew, G. (2020). The work of hermeneutic phenomenology. International Journal of Qualitative Methods, 19. https://doi.org/10.1177/1609406920947600
- Suneel, I., Saleem, S., & Mahmood, Z. (2020). Mental health functioning of adult children of alcoholic fathers in Pakistan. Rawal Medical Journal, 45(1), 140-143. https://www.rmj.org.pk/?mno=47507
- Taherdoost, H., Sahibuddin, S., & Jalaliyoon, N. (2022). Exploratory factor analysis: Concepts and theory. Advances in Applied and Pure Mathematics, 27, 375-382. https://hal.archives-ouvertes.fr/hal-02557344/document
- Thein, K. Z. K., Herberholz, C., Sandar, W. P., & Yadanar. (2021). Caring for persons with drug use disorders in the Yangon Region, Myanmar: Socioeconomic and psychological burden, coping strategies and barriers to coping. PLoS One, 16(10), e0258183. https://doi.org/10.1371/journal.pone.0258183
- Tracy, K., & Wallace, S. P. (2016). Benefits of peer support groups in the treatment of addiction. Substance Abuse and Rehabilitation, 7, 143-154. https://doi.org/10.2147/SAR.S81535
- VanDerNagel, J. E., van Duijvenbode, N., Ruedrich, S., Ayu, A. P., & Schellekens, A. F. (2018). The perception of substance use disorder among clinicians, caregivers and family members of individuals with intellectual and developmental disabilities. Journal of Mental Health Research in Intellectual Disabilities, 11(1), 54-68. https://doi.org/10.1080/19315864.2017.1390712
- Wallace, R. J. (2019). Trust, anger, resentment, forgiveness: On blame and its reasons. European Journal of Philosophy, 27(3), 537-551. https://doi.org/10.1111/ejop.12485
- Weinandy, J. T. G., & Grubbs, J. B. (2021). Religious and spiritual beliefs and attitudes towards addiction and addiction treatment: A scoping review. Addictive Behaviors Reports, 14, 100393. https://doi.org/10.1016/j.abrep.2021.100393
- Wogen, J., & Restrepo, M. T. (2020). Human rights, stigma, and substance use. Health and Human Rights, 22(1), 51.
- Yaqub, F. (2013). Pakistan's drug problem. The Lancet, 381(9884), 2153-2154. https://doi.org/10.1016/S0140-6736(13)61426-9
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.