Abstract
The use of psychoactive substances is a major global public health issue with profound physical, mental, and social consequences for individuals and their communities. Dialectical behavior therapy and acceptance and commitment therapy have gained recognition as effective interventions for addressing problematic substance use and associated emotional challenges. This case study details a 26-year-old Colombian patient with a history of problematic use of cannabis, cocaine base, and heroin, presenting with primary concerns including severe emotional dysregulation, experiential avoidance, and difficulties in maintaining social relationships. A unique aspect of this case is the application of an integrated dialectical behavior therapy and acceptance and commitment therapy treatment program, specifically tailored to Colombian cultural factors, targeting both substance use behaviors and emotional challenges. The treatment program included dialectical behavior therapy skills training to manage emotional dysregulation and reduce impulsive behaviors, combined with acceptance and commitment therapy–based techniques to enhance psychological flexibility and decrease experiential avoidance. Clinically, the patient exhibited significant improvements in emotional regulation and a reduction in substance use frequency. These changes, along with improved social functioning, emphasize the efficacy of this culturally adapted approach. This case contributes to the existing literature by demonstrating the adaptability and effectiveness of dialectical behavior therapy and acceptance and commitment therapy in treating substance use disorders within a Colombian context. It highlights the importance of cultural adaptations in therapeutic methods and sets a foundation for future studies. However, the descriptive nature of this case study and its inherent limitations regarding generalizability should be taken into account. Continued research with more rigorous methodologies is essential to validate and expand upon these findings, ensuring broader applicability across similar populations.
Keywords: acceptance and commitment therapy, case study, dialectical behavioral therapy, experiential avoidance, psychoactive substance abuse
Main Points
- Integrated application of dialectical behavior therapy and acceptance and commitment therapy in the Colombian cultural context.
- Reduction of psychoactive substance use.
- Reduction of emotional dysregulation and psychological inflexibility associated with addiction.
- Impact of traumatic experiences on the etiology of substance use.
Introduction
Substance use is a global public health challenge, with a devastating impact on those affected. According to the United Nations Office on Drugs and Crime’s World Drug Report 2023, 296 million people reported using drugs in 2021, representing a 23% increase over the previous decade. Among them, 39.5 million are diagnosed with psychoactive substance use disorders, a 45% increase in just 10 years. Additionally, 13.2 million people reported having injected drugs, representing an 18% increase by 2021 compared with previous data (UNODC, 2023).
From a transdiagnostic perspective, the pattern of behavior associated with the use of psychoactive substances is characterized by actions that produce both negative consequences and benefits for the user. One of the sustaining factors identified in addictive behavior is that the effects of the substance provide relief from the discomfort of negative experiences, unpleasant emotions or physiological sensations, and distressing thoughts. The persistent use of psychoactive substances is reinforced by negative reinforcement mechanisms, perpetuating a cycle of both physical and psychological dependence (Michałowska & Cheć, 2024). These behaviors, which involve fleeing from or rejecting inner experiences, are known as experiential avoidance (Krotter et al., 2024).
Emotional dysregulation refers to the inability to experience and regulate emotions (Linehan et al., 1999). This vulnerability factor can lead individuals to adopt harmful and rigid strategies for coping with emotional distress, thereby increasing the likelihood of psychoactive substance use, abuse, or dependence (Michałowska & Cheć, 2024). According to Linehan, dialectical behavior therapy (DBT), originally designed for the treatment of borderline personality disorder, has emerged as a promising intervention for treating psychoactive substance use. Dialectical behavior therapy combines cognitive and behavioral strategies with a dialectical approach that fosters both acceptance and change. This integrative approach allows for the addressing of emotional vulnerability, patterns of addictive behavior, and emotional dysregulation, central phenomena in the etiology and maintenance of substance use (Linehan et al., 1999).
Additionally, acceptance and commitment therapy (ACT) has demonstrated efficacy across a wide range of mental health conditions, including anxiety, depression, and substance abuse (Krotter et al., 2024). Acceptance and commitment therapy focuses on enhancing psychological flexibility through its core components: acceptance to reduce experiential avoidance, cognitive defusion, the concept of self as context, contact with the present moment, values-based living, and committed action. For substance use interventions, third-generation therapies, including ACT, have been shown to reduce impulsive behaviors, improve emotional dysregulation, alleviate suffering, and reduce addictive behaviors (Krotter et al., 2024).
Research has shown that experiential avoidance and low distress tolerance are significantly associated with substance craving in adults in residential treatment for substance use disorders; this finding suggests that addressing experiential avoidance is essential for reducing craving and preventing relapse (Shorey et al., 2017). Similarly, a study of women with substance use and borderline personality disorder found that DBT improved emotional regulation and reduced frequency of substance use; these findings support the efficacy of DBT in treating emotional dysregulation and addictive behavior (Axelrod et al., 2011). On the other hand, a study of an ACT-based programme aimed at reducing destructive experiential avoidance behaviors, including self-harm and addictions, showed significant reductions in the frequency of these behaviors and improvements in participants’ quality of life (Na et al., 2022). In the same vein, a recent exploratory review highlights the therapeutic potential of third-generation therapies, such as DBT and ACT, to address psychoactive substance use among adolescents, highlighting their focus on acceptance, psychological flexibility, and emotional regulation as key elements of effective treatment (Sequeda et al., 2024). In summary, CBT and ACT have a growing body of scientific evidence to support their effectiveness in the treatment of mental health problems, including psychoactive substance use (Krotter et al., 2024; Linehan et al., 1999).
Although studies have examined the efficacy of DBT and ACT in the treatment of emotional dysregulation and substance use, most have been conducted in cultural contexts different from that of Colombia, and the application and adaptation of these therapies in Colombia has not been sufficiently studied. Therefore, the present study aims to evaluate the effectiveness of DBT and ACT in reducing experiential avoidance, improving emotional regulation, and decreasing psychoactive substance use in a Colombian population. In doing so, the aim was to provide evidence for the applicability of these interventions in specific cultural contexts and contribute to the development of third-wave therapy-based strategies in Latin America.
Case Presentation
A 26-year-old male, who has been homeless for 6 years, is a high school graduate with unfinished higher education. He presents with age-appropriate language and memory but exhibits impulsivity, emotional lability, irritability, and inattention. He has been diagnosed with hepatitis C. His medical history reveals 13 years of problematic use of marijuana, cocaine base, and heroin. Throughout the treatment program, he has undergone rehabilitation in a psychiatric hospital, detoxification for 1 month, and psychiatric and psychological treatment for 2 months.
The patient’s father used marijuana and sold psychoactive substances, while the mother had alcohol-related issues. He grew up in a dysfunctional family with an authoritarian upbringing, experiencing domestic abuse and witnessing physical violence between his parents.
In terms of psychosocial factors, the patient lacked a stable support network, faced housing instability, poor nutrition, and significant financial difficulties. He was involved in delinquent groups and participated in illegal activities. He has been admitted three times to rehabilitation programs at a psychiatric hospital for substance abuse, each for 2 months.
Clinical Findings
The patient underwent a comprehensive assessment by the medical, psychiatric, and psychological team at the psychiatric hospital where he was admitted. A structured psychiatric assessment was carried out to assess his mental health, including symptoms of impulsivity, emotional lability, irritability, and inattention. His 13-year history of substance use disorders, including marijuana, cocaine base, and heroin, was carefully reviewed. During his hospitalization, he received psychiatric treatment, including methadone and cognitive behavioral therapy, to address his addiction and emotional dysregulation.
In addition to psychiatric care, a thorough medical assessment was carried out. The patient was diagnosed with hepatitis C, a condition with significant health implications. He was also moderately malnourished, with a body mass index below average for his age and height, probably due to prolonged drug use and homelessness. Physical signs of intravenous drug use were evident, with track marks on his arms. In addition, symptoms of physical anxiety were observed, such as mild hand tremors, excessive sweating, and psychomotor restlessness, particularly in stressful situations.
Psychologically, the patient’s cognitive and emotional functioning was assessed. His memory and language were found to be appropriate for his age, but his cognitive performance fluctuated due to impulsivity and emotional instability. Although his speech was coherent, he showed considerable irritability and emotional lability during the interview. His psychosocial history revealed a lack of a stable support network, exposure to domestic violence, and involvement in illegal activities, which further contributed to his emotional and behavioral difficulties.
Pharmacological Treatment
During his hospitalization and rehabilitation, the patient received pharmacological treatment aimed primarily at managing withdrawal symptoms, reducing cravings, and stabilizing his emotional and behavioral dysregulation. As part of his psychiatric treatment, he was given methadone therapy, a standard medication for opioid dependence, which helped to alleviate withdrawal symptoms and reduce cravings for heroin. He was also prescribed psychiatric medications to treat emotional instability, impulsivity, and irritability, including valproic acid and quetiapine.
The patient showed some positive effects of the pharmacological treatment, such as a temporary reduction in drug craving, improved emotional regulation, and increased engagement in psychological therapy. However, some side effects were observed, including mild hand tremor, excessive sweating, and psychomotor agitation, especially under stress, which may be related to withdrawal symptoms or medication use.
The timeline shows how traumatic factors and adversities, such as domestic violence, sexual abuse, and early substance use, marked the patient’s life since childhood. These events contributed to the development of problematic substance use, accompanied by housing instability and criminality. The patient faces relapses and intermittent treatment.
Diagnostic Assessment
The study used a single-subject ABA (Applied behavioral analysis) case design, with the intervention as the independent variable and experiential avoidance, emotional dysregulation, and psychoactive substance use as dependent variables. These were assessed through quantitative data from instruments and subjective reports from the participant.
Acceptance and Action Questionnaire-II (AAQ-II) (Ruiz et al., 2016): Measures experiential avoidance and cognitive inflexibility. A score above 30 indicates clinical issues, with an internal consistency of 0.93.
Cognitive Fusion Questionnaire (CFQ) (Ruiz et al., 2017): Assesses cognitive fusion. A score of 29 or higher indicates clinical difficulties, with an internal consistency of 0.95 in Colombia.
Brief Experiential Avoidance Questionnaire (BEAQ) (Vázquez-morejón et al., 2019): Measures experiential avoidance on a 6-point Likert scale. Higher scores indicate more avoidance, with an internal consistency of 0.82.
Drug Abuse Screening Test (DAST-10) (Pérez et al., 2010): Detects problematic substance use. A score of 1–2 indicates low use, 3–5 moderate, 6–8 substantial, and 9–10 severe. It has an internal consistency of 0.93.
Emotional Regulation Assessment Scale (DERS) (Bohórquez-Borda et al., 2023): A 36-item scale assessing emotional regulation across six factors, with an internal consistency of 0.93 and test-retest reliability of 0.88.
Procedure
The psychological assessment involved operationalizing the reason for consultation, conducting synchronic and diachronic analyses, and evaluating the contexts of functioning based on the clinical case formulation model. CAse REport guidelines were implemented in order to rigorously report the case report (Gagnier et al., 2013). The procedure included two assessment sessions (interview and administration of instruments) and 6 intervention sessions (see Table 1).
| Table 1. Patient’s alcohol, smoking, and substance involvement screening test results | ||
| Type of Psychoactive Substance |
|
Risk Level |
| Alcohol |
|
Low |
| Amphetamine-related stimulants |
|
Low |
| Inhalants |
|
Low |
| Cannabis |
|
Moderate |
| Sedatives or hypnotics |
|
Moderate |
| Cocaine |
|
Moderate |
| Opioids |
|
High |
| Others (cocaine base) |
|
High |
Initial Assessment Findings
Synchronous analysis: The patient exhibited problematic use of multiple psychoactive substances, engaged in criminal and illegal behavior, and utilized homosexual relationships to obtain economic resources. He exhibited signs of emotional dysregulation, including thoughts of guilt, rejection, resentment, and hatred toward his mother figure. Additionally, he experienced recurrent thoughts of failure and difficulties with self-esteem. He also lacked a family and social support network (see Table 2).
| Table 2. Risk Indicators of emotional dysregulation, experiential avoidance, and psychoactive substance abuse in patients Q1 | ||
| Emotional Dysregulation | Experiential Avoidance | Abuse of Psychoactive Substances |
| Emotional lability | Dissociation | Illegal behaviors |
| Sense of hopelessness | Family isolation | Violent acts toward self and others |
| Feeling of emptiness | Substance use to alleviate emotional distress | Risky sexual relations |
| Nonacceptance | Low enjoyment of leisure activities | Homeless |
| Depression and anxiety | Difficulty in making decisions | Problematic social relationships |
| Aggressiveness and impulsivity | Substance use in response to stress, interpersonal conflicts, or excessive responsibilities | Sudden changes in behavior |
| Interpersonal conflicts | Substance use to eliminate painful childhood memories | Troubled romantic relationships |
| Absence of coping strategies | Frequent verbal and behavioral manifestations of distress caused by emotions | Incidence of diseases associated with consumption |
| Low emotional identification | Difficulty in the enjoyment of daily activities | Distancing from valuable goals |
Diachronic analysis: The patient experienced multiple traumatic situations. He was involved in his father’s illegal activities (drug dealing, arms dealing), witnessed the murder of his father when he was 9 years old, watched his mother engage in sex work, encountered problematic alcohol consumption by his parents, and was the victim of extreme physical violence by his mother. At the age of 14, he was repeatedly sexually abused by different perpetrators.
Alcohol, smoking, and substance involvement screening test (ASSIST) (Valladolid et al., 2014). This test is designed to detect substance use and abuse. It identifies levels of risk associated with substance use and determines the most appropriate care based on the individual’s results. Scores are classified as follows: low risk for alcohol (0–10 points) and other substances (0–3 points), moderate risk for alcohol (11–26 points) and other substances (4–26) points, high risk for alcohol (27 or more points) and other substances (27 or more points). It is important to note that although ASSIST includes questions about tobacco use, this is for screening purposes only, and no risk level is assigned to tobacco. The ASSIST has an internal consistency ranging from 0.55 to 0.74 and test-retest reliability ranging from 0.58 to 0.91. The results are presented below.
There is evidence of a high risk for the use of cocaine base and opiates such as heroin, as well as a moderate risk for the use of cannabis, tranquilizers, and cocaine. However, there is a low risk for the use of alcohol, amphetamines, and inhalants.
Adverse Childhood Experiences International Questionnaire (ACE-IQ): This tool measures adverse childhood experiences, including family dysfunction, abuse, physical, sexual, or emotional neglect, peer violence, exposure to violence, substance abuse by caregivers, deceased or separated parents, and other adverse experiences in individuals older than 18 years (World Health Organization, 2018). The current study utilized the binary response form.
In evaluating adverse experiences before the age of 18, the patient reported experiencing the violent loss of his father, living with a depressed mother who attempted suicide, encountering alcohol and drug problems, witnessing violence between his parents, having an uncle who went to prison, being subjected to insults, belittlement, and beatings by his mother and relatives, feeling unloved by his family, and experiencing unwanted sexual contact. In the clinical assessment, the patient rated these events as having “greatly” affected his health development. The patient reported 12 out of 14 adverse childhood experiences related to violence, family dysfunction, psychological abuse, physical abuse, neglect, and sexual abuse.
Therapeutic Intervention
The intervention scheme was an adaptation of the DBT strategies, as outlined by Linehan et al. (1999), and ACT strategies, as described (Hayes et al., 2011), specifically tailored for psychoactive substance use/consumption disorders accompanied by emotional dysregulation and experiential avoidance. The treatment included three components: individual therapy strategies (Table 1), building a social support network (through institutional resources and friendships), and the use of pharmacotherapy as a drug substitution (involving interdisciplinary interventions from psychiatry).
The individual assessment and intervention program was conducted over eight sessions (see Table 3). The findings of the intervention are detailed below:
| Table 3. Description of sessions with substance use patients | ||
| Session No. | Therapeutic Technique | Description |
| 1 | Pre-treatment phase (commitment and clarification of values) | The first session addressed the phases of the therapeutic process, facilitating a safe and validating space where she could feel heard without judgment. The session opened with a warm welcome and a brief exploration of his current mental and emotional state, reinforcing the importance of his presence as a first act of courage and commitment to his mental health. From the dialectical approach of dialectical behavior therapy (DBT), a therapeutic posture was sustained that balanced the validation of his suffering with openness to the possibility of change, modeling from the beginning the dialectical attitude of the intervention. |
|
The informed consent form was read and signed, explaining clearly and respectfully the ethical conditions of the accompaniment, the limits of confidentiality, the role of the therapist, and the expectations of the process. The therapeutic contract was then established, defining key aspects such as attendance, duration of sessions, commitment to tasks between sessions, and responsible communication in case of possible crises. At this point, from acceptance and commitment therapy (ACT), the idea was introduced that the commitment is not to the therapist, but to a more meaningful life aligned with her values, even if that means going through discomfort. |
||
| Subsequently, the functional assessment of the problem was initiated by conducting a detailed chain analysis of the drinking behavior. Triggering events, previous contextual vulnerabilities (such as family arguments, insomnia, hunger), associated emotions and thoughts, the drinking behavior itself, and the immediate and long-term consequences were explored. This was developed through open-ended questions and empathic validation. The patient was able to identify how consumption emerged as a strategy to regulate intense emotions such as anger, frustration, or sadness, even if in the long term it generated guilt, isolation, and loss of personal goals. | ||
| Throughout the analysis, the concept of experiential avoidance, one of the central processes in ACT, was introduced experientially. To facilitate its understanding, the metaphor of the “man in the hole” was used, helping him to visualize how, in a desperate attempt to escape from the discomfort, there was a man in a hole, who in order to get out dug deeper and to try to fight his way out, the opposite happened, the hole got bigger. This metaphor served as a bridge to introduce the logic of the ACT model: it is not about eliminating the discomfort, but to stop fighting with it and learn to move forward with it present, committing to actions guided by its values. | ||
|
Dialectical behavior therapy and ACT concepts such as emotional dysregulation, validation and training in specific skills (mindfulness, emotional regulation, distress tolerance, and interpersonal effectiveness) were explained. From ACT, the hexaflex model was explained through highlighting the processes of defusion, acceptance, values clarification, and engaged action. To illustrate cognitive fusion—another key process in ACT—the metaphor of the “mental radio on” was used, allowing the patient to identify how their thoughts are often imposed as absolute truths that determine their behavior, without questioning or distance. After psychoeducation, a space for dialogue was opened to evaluate the willingness to change, asking gently what emotions and thoughts he has tried to avoid, what strategies he has used to do so, and what consequences this has brought him in his life. The value dimension was also explored, introducing questions aimed at clarifying what is important to him, even in the midst of pain. This exercise allowed to open a small crack in intrinsic motivation, by connecting with the desire to rebuild the link with his family, regain the trust of his environment, and resume personal projects interrupted by consumption. To conclude, the first therapeutic objectives were agreed upon: to reduce substance use as an automatic response to emotional distress, to learn new emotional coping strategies, and to reconnect with a meaningful life project. A homework assignment was left between sessions to start a record of significant events where she experiences emotional distress, recording thoughts, emotions, and associated behaviors. |
||
| 2 | Psychometric assessment (ACT functional contextualization phase) |
In this session, clinical instruments were applied with the aim of deepening the functional understanding of the case, identifying risk factors associated with substance use, and exploring psychological processes and central variables such as experiential avoidance and cognitive fusion. A warm clinical attitude was maintained and in function of the patient’s gestures and body, taking care that the application was not experienced as an interrogation, but as a space to observe from the outside the patient’s own emotional, behavioral, and cognitive response patterns. The day began with a brief review of the previous session, reconnecting with the main ideas worked on about suffering and therapeutic engagement. Then, the purpose of the instruments was explained from a functional perspective: “To know better how you have been coping with pain, to understand what things have impacted you, and to discover what kind of thoughts or emotions trap you, in order to help you in a more precise way.” First, the ACES (Adverse Childhood Experiences Scale) was applied in order to identify traumatic experiences during childhood and adolescence that could be related to the emergence of maladaptive strategies such as consumption. This tool allowed to the open a narrative about events of abandonment, violence, and family dysfunction, not only as a clinical history, but also as part of the framework that supports the current emotional dysregulation. Subsequently, two key instruments were administered to assess the severity of substance use: DAST-10 (Drug Abuse Screening Test): It provided an objective measure of the impact and dependence generated by substances. ASSIST (Alcohol, Smoking and Substance Involvement Screening Test): Provided a broader analysis of the pattern of use and the presence of high-risk substances, making it possible to identify critical moments of relapse or greater vulnerability. The application of these scales was accompanied by an attitude of curiosity and validation, avoiding judgments but rather understanding how consumption became a way to survive emotionally. Next, deep psychological processes were explored using three tools of the ACT model: AAQ-II (Acceptance and Action Questionnaire), which measures experiential avoidance and psychological rigidity. BEAQ (Brief Experiential Avoidance Questionnaire), which allows for observing in detail the areas of life where the person has avoided feeling, remembering, or thinking. CFQ (Cognitive Fusion Questionnaire), designed to assess the level at which thoughts are taken as truths that govern behavior. These instruments allow us to explain that human beings struggle with what they feel or think, and that the important thing is not to eliminate thoughts or emotions, but to learn to relate to them in a different way. During the application, the patient was open, and the responses to the instruments evidenced relevant clinical indicators: early trauma experiences, problematic substance use, and elevated levels of experiential avoidance and cognitive fusion. These results not only provide diagnostic information but also served as the basis for a meaningful clinical conversation, in which the patient could begin to recognize how the attempt to “not feel” has kept him trapped in repetitive cycles of suffering. The session ended with a brief practice of conscious breathing (mindfulness), as a transition to work with emotional regulation skills that will be addressed in the next session. |
| 3 | Mindfulness (Mindfulness DBT) - Part I |
The third session was focused on Mindfulness skills training, a transversalaxis of both the DBT and ACT models. The main objective was to introduce the conceptual and practical bases of this skill as a means to strengthen abstinence, reduce craving, and manage the emotional discomfort that often leads the patient to experiential avoidance. The session began with a brief inquiry about recent situations of craving or emotional discomfort, validating the experience without making judgments. Questions were used such as: “What do you feel when you want to consume and cannot do it because of the hospitalization process?” or “What do you notice in your body when this happens?” This introduction opened the space to connect directly with the need to learn tools to observe internal signals without reacting to them. The patient is told the fundamental principles of Mindfulness from DBT; it was explained that there are at least three ways of relating to an experience: An emotional mind dominated by urgency, impulsiveness, and intense emotions. A rational mind that reasons and acts according to logic, without considering the emotional. And a cognizant mind that is the middle between the two previous ones; it allows one to act with balance, to consider what is felt and what is known. |
|
The metaphor of the circle of the wise mind was used, a diagram with three circles was drawn, and the patient was asked to locate a recent situation of consumption or risk, reflecting on the mental state from which he/she acted. It was practiced through an experiential exercise starting with breathing and inviting observation of the “register of sensations” with eyes closed, identifying which parts of the body were tense, which emotions were present. “Notice what happens in your body when you feel anxiety, but without trying to change it. Just observe.” Then it is directed to put the experience into words, describing it, complementing the recognition of thoughts and emotions. And to be able to recognize that it is only a thought. During the exercise, you are invited to be in contact with the present experience. After completing the exercise, the concept of radical acceptance is introduced, which is defined as the full willingness to accept reality as it is, without resistance to the experience that accompanies it. The wave metaphor was used: “Imagine you are at sea. A strong wave is approaching. You can fight it, spend all your energy … or you can float on it, even if it gets you wet. The wave can’t be stopped, but you can learn to surf it.” The patient was able to identify that, when faced with thoughts of anguish or memories of family conflict, his automatic response tended to be to consume. He recognized that these reactions were impulsive and failed to resolve the underlying distress. The session allowed the patient to make direct contact with his internal states without avoidance or judgment, introducing for the first time the experience of acceptance. A mindfulness approach was achieved, focusing on observation, reduction of discomfort, and readiness to change. |
||
| 4 | Mindfulness - Part II (Mindfulness DBT + ACT) |
The fourth session was developed in training in mindfulness skills, seeking mental openness and body observation with sustained attention without judgment, in order to strengthen the patient’s permanence in the present during his detoxification process and continue to reduce the emotional and physical discomfort that can activate his desire for the consumption behavior in the hospitalization process. To continue, the experience of the previous session is briefly taken up again. The patient reported having been able to perceive his thoughts. This positive disposition made it possible to link the previous work with the new exercises proposed. It begins by performing a breathing exercise as an attentional anchor, with the purpose of focusing the mind on the present and noticing the sensations that accompany the emotional reactivity. Giving indications such as: “feel how the air enters through your nose... and try to notice how it comes out through your mouth. Don’t try to change anything, just notice how it is.” “If your mind gets distracted, come back here and bring it back with kindness. That’s also part of the exercise.” “Every breath is an opportunity to come back.” |
|
The idea of breathing as an internal refuge was worked on, an accessible constant even in the moments of greatest tension. Clinical outcome: The patient reported that, during the exercise, he felt “as if he could release a little of the pressure of the body” and that the idea of consuming was dissolving. After this, a body scanning practice was introduced, starting from the head to the feet, inviting the patient to observe the physiological sensations, without interpreting or reacting to them. This technique allows decreasing the fusion with thoughts and increasing tolerance to physical and emotional discomfort, key in abstinence processes. The exercise was guided through the following phrases: “Place your feet in contact with the floor, assume a comfortable and attentive posture in your body,” “Bring your attention to your body,” “Bring your attention to your body,” “Take your attention to your body,” “Take your attention to your body.” “Bring your attention to your body, observe if there is tension? Just observe.” “You don’t need to do anything with what you encounter, just feel it and let it be.” “If you feel discomfort, you can notice how it changes with each breath.” At the end of the exercise, a space for reflection was opened. It was explored how it was to observe the body without making judgments or trying to control the sensations. The patient mentioned: “It is difficult … I was distracted several times, but I did manage to realize that I could stay.” His perception of the exercise is socialized by trying to resemble it with the following metaphor of the dark tunnel. “Your experience may have been similar to being in a tunnel with a shovel. And wanting to get out, you try to keep digging to the bottom, but maybe it’s not going to work. But for a moment you allow yourself to be there in that space, managing to walk, in another direction, trying to go to the place of light ahead, not behind.” Significant reduction of subjective discomfort: from an initial Subjective Units of Distress Scale (SUDs) of 9 to 1 SUDs at the beginning of the session and 4 SUDs at the end after guided practice. Increased awareness of the body and the present moment. |
||
| 5 | Emotional regulation (DBT) + values (ACT) |
In this session, the exercises that were assigned as homework in the previous session are fed back. The work session begins with a focus on emotions. The dashboard metaphor is used to open the space. After this, an attempt is made to guide the patient to a list of emotions, verifying the facts, analyzing the chain effects to invite him to improve the moment, trying to make opposite actions directed to important values of his hospitalization process. Emotions are not the problem, but often one’s relationship with them and one’s impulsive responses are. The metaphor of the emotional dashboard was worked with. It is introduced: Imagine a pilot inside an airplane, and he is inside the cockpit, and there is a dashboard indicating various alerts, for example, turbulence or storm. Now the pilot could try to act impulsively, divert his path or land from one pile to another, try to continue piloting by identifying the signal in the opposite way to those of the impulse, will be able to do it calmly even though the alert is still on and gradually on the way stabilizes. From ACT, the idea was reinforced that feeling uncomfortable emotions is not a mistake, and that it is possible to act in the direction of what one values, even in the presence of fear, anger, or sadness. Then, a checklist of emotions (anger, sadness, fear, shame, guilt, joy, etc.) is introduced, and the patient is asked to identify which ones he/she has felt most frequently. And the fact-checking strategy is practiced, which helps to distinguish between what the emotion makes us think and what really happened. Situation: “I was ignored at the group meal.” Emotion: anger. Thought: “I have to make myself respected.” Verification: “What evidence is there of that—was it an omission or an automatic interpretation?” The patient was able to recognize that he had assumed without confirming, and that, when he approached to ask, his companions responded kindly. This exercise facilitated defusion, reducing the power of automatic thoughts. The behavioral chain analysis and identification of the point of intervention are done in sequences so that you can see where the impulsive behaviors (isolation, emotional explosion, consumption) come from. A table was made to see the situation, his vulnerability, such as disturbed sleep, thoughts of worthlessness, the intense emotion: anger, and the problem behavior of disconnection, escape, desire to consume, in order to be able to guide him to alternative strategies. The opposite action skill was trained, explaining that when an emotion invites you to impulsive actions, change can be generated by acting in the opposite direction to what the emotion calls for. |
|
One activity put into practice was that “faced with the annoyance with his peers and the assigned tasks, he chose to collaborate in cleaning the animal room with the strategies used in What and How” and acknowledged that although at first he did not want to, at the end of the activity, he felt calmer and more connected. It was observed how the patient was able to relate recent situations where he used problem-solving and emotional regulation strategies, such as taking distance, breathing, writing, or talking to a partner. In session No. 5, a significant decrease in subjective distress was observed: she went from 9 to 1 on the SUDs scale, she improved her strategies for understanding the opposite action, and she solved conflicts by better managing her emotions, thoughts, and behavior in context. |
||
| 6 | Discomfort tolerance (DBT) + Acceptance (ACT) |
The session began by recognizing that experiencing emotional pain is an inevitable part of life, but that it is possible to learn to move through it without reacting impulsively or destructively. The metaphor of “passengers on the bus” was introduced to simulate the experience in the presence of disturbing memories, thoughts, and emotions, without the need to stop and fight with them, but to allow ourselves to be in contact and take distance. From this framing, practical DBT skills were trained, including the STOP skill, a core strategy of DBT for managing crises without acting impulsively. This tool was presented as a sequence that allows gaining time and clarity before reacting. First, the S - Stop step was worked on, teaching the patient to stop physically and mentally in situations of high emotional charge, avoiding saying or doing something immediately. Then - Take a step back was practiced, guiding the patient to take a step back, both literally and symbolically, to observe the situation from a greater emotional distance. Next, O - Observe was applied, promoting full awareness of thoughts, emotions, physical sensations, and environmental cues, using questions such as, “What am I feeling?”, “What is happening in my body?”. And then guided to P - Proceed mindfully, inviting you to act with mindfulness, choosing a response aligned with what is important to the recognized self, rather than being driven by impulse. After this exercise was developed, the next strategy, known as “IMPROVE,” was introduced through an experiential exercise designed to help in facing crises. The strategy begins with guided phrases, inviting you to: “close your eyes and allow your breathing to find its natural rhythm. Imagine a place where you feel completely safe, calm, protected; it can be real or invented—a cozy room, a view of the sea— let your mind go through it calmly (I). Now, while you stay in that place, ask yourself: what is the meaning of this difficult moment I am going through, can it be an opportunity to grow, to take care of myself, to become stronger (M)? Repeat in your mind compassionate phrases: ‘I am doing the best I can in this moment,’ ‘I can feel this without letting it destroy me,’ ’I am more than this emotion’ (P). Now bring your attention to your body: inhale deeply, release the air slowly, feel how the body begins to relax. If you wish, you can slightly move your shoulders, neck, or rub your hands to release tension (R). Remember that you don’t need to solve everything now: just take a small step, one that is within your reach today, such as talking to someone, taking a walk, or resting for a moment (O). Reconnect with what really matters to you: what do you want to take care of right now: compassion, stability, respect, freedom? Allow yourself to feel that acting on what is important to you is also a way to move forward (V). Finally, come back to this space little by little, open your eyes, and try to observe with your senses: notice 3 objects that you see, notice 2 sounds that you hear, 1 that you can touch, 1 that you smell. This moment is yours, you can be with it without running, without fleeing (E). Breathe calmly again, and when you are ready, open your eyes slowly.” This activity allowed her to experience a noticeable decrease in discomfort, going from a SUDs of 9 to 4. During the session, the patient expressed feeling more prepared to face moments of discomfort. At this point in the intervention, the patient showed a high level of commitment to put the skills into practice, improvement at the emotional level, and the willingness and openness to the process of hospitalization and discharge from the clinic. |
| 7 | Interpersonal effectiveness (DBT) + Values commitment (ACT) | The session focused on interpersonal effectiveness skills training, a fundamental component of the DBT model to strengthen relationships, reduce social pressure, and prevent relapse associated with the environment. From an experiential perspective, concrete skills were taught to improve communication, set boundaries, and resolve conflicts without giving in to intense emotions or avoiding their emotions as a function of their relationships. Two key strategies were introduced and practiced: DEAR MAN (Describe, Express, Affirm, Reinforce, Maintain posture, Appear confident, Negotiate) to ask for what is needed in a firm and clear way, and GIVE to maintain relationships with respect and empathy (Be gentle, Show interest, Validate, Maintain balance). |
|
The session focused on interpersonal effectiveness skills training, a fundamental component of the DBT model to strengthen relationships, reduce social pressure, and prevent relapse associated with the environment. From an experiential perspective, concrete skills were taught to improve communication, set boundaries, and resolve conflicts without giving in to intense emotions or avoiding their emotions as a function of their relationships. Two key strategies were introduced and practiced: DEAR MAN (Describe, Express, Affirm, Reinforce, Maintain posture, Appear confident, Negotiate) to ask for what is needed in a firm and clear way, and GIVE to maintain relationships with respect and empathy (Be gentle, Show interest, Validate, Maintain balance). Describing: “You’re telling me to run away from the center to the trees to get down mangoes,” He continued with Expressing: “That makes me uncomfortable because I’m trying hard to stay in the process and follow the rules,” then he affirmed his decision: “I’m not going to do it, I don’t want to go backwards or negative consequence in my process,” He reinforced: “I prefer to keep moving forward, I have felt better since I have been recognized as a leader in the hospitalization process.” Maintained the stance, not giving in, even if the other insisted. Appeared confident, avoiding defensive or aggressive reactions, and negotiated an alternative way out of the situation: “If you need to distract yourself, we can do something that doesn’t involve breaking the rules, like playing some sports on the court.” In addition, the GIVE skill was integrated: the patient was gentle, using a calm tone, showed interest in the other’s discomfort (I understand that you are bored and very hungry, also a little frustrated), validated emotions (sometimes we all want to escape for a while, I have also gone through that and breaking the rules can be striking), and maintained a balance between taking care of his process and not deteriorating the social bond. The patient expressed feeling important, achieving to be learning strategies and recognizing that “before I would have let myself go and I would have done it, other times I would have been very aggressive, but for me it is more important to stay well in this process.” Through role-playing, the patient rehearsed difficult conversations with his group mates, authority figures within the center of specialization, and also role-played with his family members, applying these skills in simulated situations that reflected real conflicts. Special work was done on identifying signs of social pressure related to consumption, and assertive responses were elaborated, as well as situations where the family may deny their support when leaving the institution. Work was done on letters with therapeutic accompaniment, communicating progress and requesting support, applying emotional validation skills, and clear communication. These interventions reinforced the family bond as a support network and allowed the patient to accept the limitations of his family context once he left the clinic, while strengthening the perception of interpersonal self-efficacy and resilience. The patient was able to identify recent situations in which he was able to set limits and express his needs. A significant decrease in interpersonal discomfort was observed, going from an initial SUDs of 9 to 3 at the end of the session, accompanied by verbalizations that reflect greater security, assertiveness, and autonomy: “I no longer feel obliged to say yes so that they don’t get angry or accept the answer and reach agreements.” This session was key to consolidating behavioral change in her social context, allowing her to act from her values and recovery goals, even in complex relational environments. |
||
| 8 | Follow-up and closure (ACT maintenance phase + DBT generalization) | In the follow-up and closure session, held 3 months after the end of the intervention process, a comprehensive review of the patient’s progress was carried out, evaluating not only his or her current state but also the challenges faced after leaving the clinical setting. The session began with the application of post-treatment instruments used in previous phases, which allowed contrasting indicators of change in variables such as experiential avoidance, cognitive fusion, and risk of relapse. The results, together with the patient’s own account, evidenced maintenance of abstinence in the use of psychoactive substances, as well as a greater capacity to identify, accept, and regulate difficult emotions without resorting to impulsive behaviors. The patient shared that, in everyday situations such as family conflicts or work tensions, he has been able to apply learned strategies, such as the opposite action, the use of DEAR MAN in difficult conversations, and the practice of mindfulness to not let himself be dragged down by the discomfort. For example, she recounted how, upon receiving unfair criticism from her mother via telephone, who is a family member who distrusts her process, she managed to stop, validate her emotion, and respond firmly but respectfully, avoiding further conflict and ending the call. He also expressed having faced thoughts of hopelessness and desires of avoidance, but was able to observe them and distance himself, using defusion exercises and contact with his purpose of graduation, of getting ahead, being recognized, and helping others. In this session, the achievements were reinforced, the sustained commitment to recovery was validated, and practical guidelines were offered for ongoing risk management, a relapse prevention plan, identification of early signs of emotional vulnerability, and the conscious use of support networks were made in the middle of the session. A compassionate view of relapses as part of the learning process, not as failures, was promoted. The patient ended the session with a SUDs discomfort score of 4, significantly lower than at the beginning, and verbalized feeling that he had the tools to sustain his recovery path, with several activities and action plans to help other people going through addiction processes and the intention of being part of an institution as a support network in the accompaniment processes. This session closed the process with a sense of continuity and autonomy, integrating the therapeutic experience into their daily life with greater acceptance, responsibility, and connection with their life purpose. |
Follow-Up and Outcomes
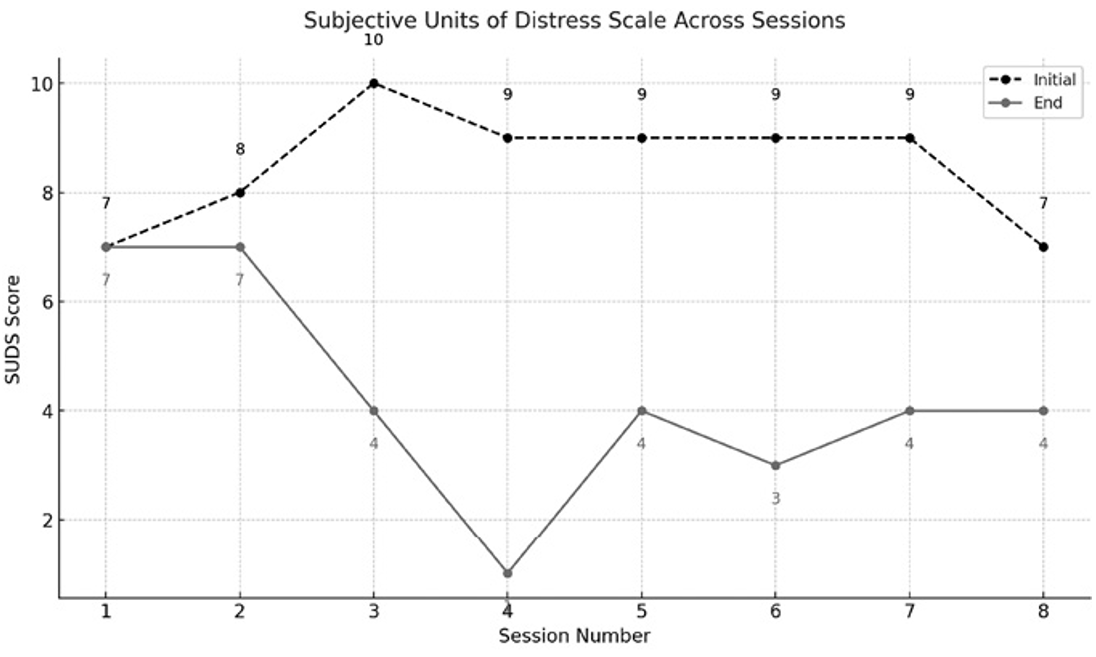
This case study analyzes the effects of a culturally tailored DBT and ACT treatment program for psychoactive substance abuse, emotional dysregulation, and experiential avoidance in a patient with a clinical history. The results offer insights into the applicability and effectiveness of these therapies in the Colombian context and provide guidance for addressing substance abuse, emotional dysregulation, and avoidance. Figure 1 shows the “Subjective Units of Distress Scale” (SUDS) at two time points: initial and end of the session, with the black line representing initial values and the gray line showing post-intervention values (see Table 4).
| Note: AAQ-II = Acceptance and Action Questionnaire-II; ACES = Adverse Childhood Experiences Scale; ASSIST = Alcohol, smoking, and substance involvement screening test; BEAQ = Brief Experiential Avoidance Questionnaire; CFQ = Cognitive Fusion Questionnaire; DAST-10 = Drug Abuse Screening Test; DEAR MAN = Describe, Express, Affirm, Reinforce, Maintain posture, Appear confident, Negotiate; DERS = Difficulties in Emotion Regulation Scale; SUDs = Subjective Units of Distress Scale. | ||||||
| Table 4. Intervention program for the treatment of substance use, experiential avoidance, and emotional dysregulation | ||||||
| Session No. | Therapeutic Technique | Description | Session Duration |
|
Findings of the Intervention | |
|
|
|
|||||
| 1 | Pre-treatment phase |
Application of informed consent and therapeutic contract. Initial evaluation of the problem is performed with functional and chain analysis. Therapy theory guide. Experiential avoidance is assessed. Goals, rules, and commitments to the therapeutic process are defined, and readiness for change is assessed. |
2 hours |
|
|
The patient is motivated, cooperative, and committed to the process. The patient voluntarily agrees to participate in the psychological assessment and intervention. The patient is observed as having functional cognitive abilities to understand each phase of treatment. |
| 2 | Instrument application |
The application of ACES to evaluate traumatic experiences. DAST-10 and ASSIST to assess the level of risk of use. AAQ-II, BEAQ, and CFQ to assess experiential avoidance and cognitive fusion. |
1 hour |
|
|
The results reflect clinical indicators for each of the variables assessed (see ). |
| 3 | Mindfulness (first half) | The principles of mindfulness, behavioral dialectics, and radical acceptance are addressed. Mindfulness training is offered to observe, describe, and participate in the present to help maintain abstinence, reduce craving, and manage the emotional discomfort that leads to experiential avoidance. | 1 hour |
|
|
Signs of substance use risk are i dentified. Mindfulness strategies are used to observe them without judgment or automatic reaction, which helps to avoid dropping out of rehabilitation. Finally, emotional and physical discomfort is reduced, which is confirmed by measuring SUDs. |
| 4 | Mindfulness (second half) | Instructions are given to focus attention and mental openness through breathing. The body is scanned for physiological sensations without judgment. | 1 hour |
|
|
There is evidence of increased awareness of the present during detoxification, improved adherence to therapeutic rules and coexistence, and reduced avoidance of unpleasant experiences, thoughts, and emotions. |
| 5 | Emotional Regulation | Emotion function and response were addressed using metaphors, an emotion checklist, and fact checking, and chain behavior was analyzed to reduce impulsive action. In addition, to effectively modify the patient’s emotions, appraisal of emotional reactions was coached, and the opposite action was practiced. | 2 hours |
|
|
The patient displayed appropriate strategies to regulate emotions and behaviors, responding in the opposite way in challenging situations (e.g., he would go with his peers to clean out the animal room). He used problem-solving strategies, counteractions, and regulated emotions, thoughts, and relationships with the context. |
| 6 | Tolerance to discomfort- distress | The session focused on distress tolerance through the use of gradual exposure to trigger stimuli and the use of radical coping and acceptance skills training. Role-playing and metaphors were used to prevent avoidance and improve self-compassion. The “IMPROVE” tool was taught to manage crises and possible relapses through emotional regulation and sensory exploration. | 2 hours |
|
|
The patient acquires tools to manage discomfort (P, C, E), reduce side effects, and reports peace of mind by using the “IMPROVE” tool to explore sensory experiences. |
| 7 | Interpersonal effectiveness | Effective skills for healthy relationships and for reducing the use of psychoactive substances are taught. Role-playing is used to teach assertive communication skills, limit setting, conflict resolution, and negotiation. Calls are also made to family members to report progress and increase family support, and communication strategies and emotional validation are taught. DEAR MAN and GIVE strategies are used to reinforce effective communication. | 2 hours |
|
|
There is evidence of improved interpersonal relationships, setting limits, resolving conflicts, and communicating with peers and therapists. There is evidence of a reduction in social pressure to return to drug use. |
| 8 | Follow-up and closure | Follow-up and closure 3 months after completion of the intervention, post-treatment instruments are administered. Challenges that the patient has encountered in the treatment process are evaluated. Guidelines are given to continue to manage the patient’s problems and avoid relapses. | 2 hours |
|
|
Displays commitment to rehabilitation and recovery. Abstinence from psychoactive substance use, improved ability to regulate emotions, cope with daily challenges, and feelings of frustration. Greater acceptance of thoughts, feelings, and sensations, i.e., less experiential avoidance. Improved interpersonal relationships. |
From the patient’s perspective, noticeable changes occurred in their emotional and cognitive experience during therapy. Initial scores ranged from 7 to 10 (mean = 8.5, standard deviation [SD] = 1.3), whereas at the end of the intervention, scores decreased to a range of 1–8 (mean = 4.8, SD = 2.3), reflecting a marked reduction in subjective distress. As shown in Table 2, the SUDs scores indicate a high and relatively stable level of discomfort at baseline, followed by a substantial decrease by the end of treatment, suggesting clinically meaningful improvement in the patient’s psychological state.
Assessment tools were used to measure aspects related to substance use, emotional regulation, and experiential avoidance. Pre- and post-intervention results across measurement scales are presented in Table 2 and illustrated in Figure 2, highlighting changes in the patient’s evaluation over time.
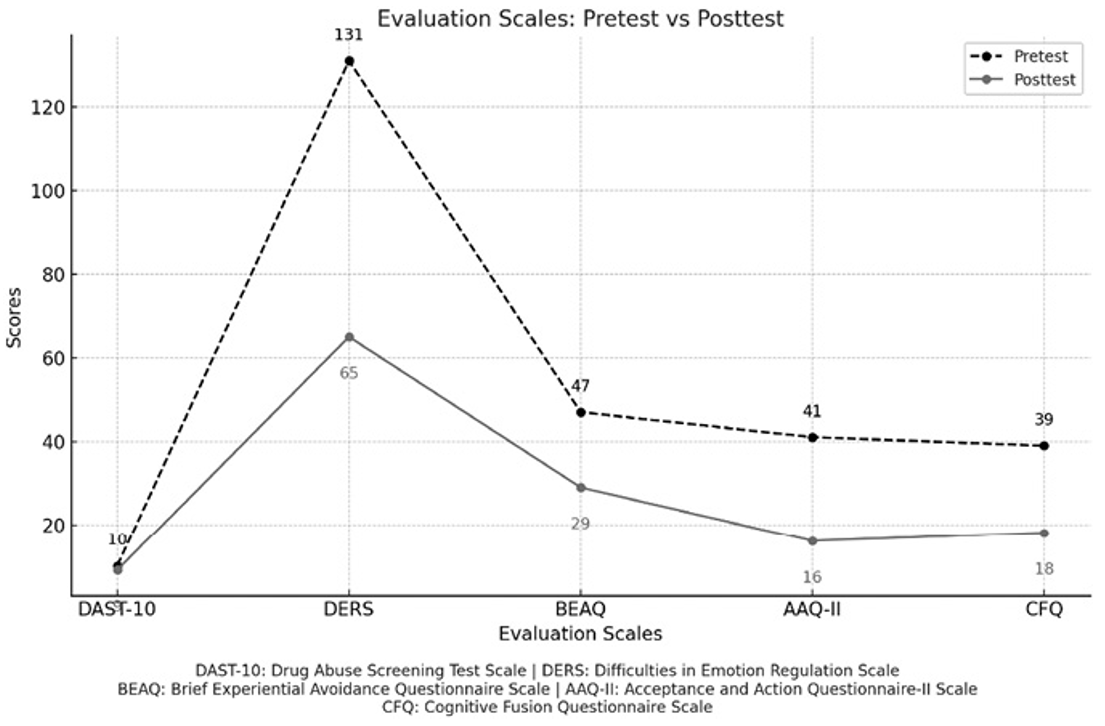
The changes observed in the initial and final scores on the various scales suggest improvements in the symptoms assessed, especially in emotional regulation and in the reduction of experiential avoidance. The scores on the scales appear to show a decrease in the patient’s initial difficulties, reflecting a positive response to DBT and ACT-based treatment.
The scores from the AAQ-II (Ruiz et al., 2016) (initial 41, final 16) and BEAQ (Vázquez-Morejón et al., 2019) (initial 47, final 29) reflect a decrease in experiential avoidance and an increase in emotional acceptance. The patient demonstrated a willingness to face emotions without resorting to psychoactive substances. The AAQ-II indicates increased psychological flexibility, adopting healthier behaviors in response to distressing cognitions. The CFQ results (initial 39, final 18) suggest a greater ability to observe thoughts objectively.
In the DERS (Bohórquez-Borda et al., 2023), the patient improved from 131 to 65, indicating better emotion management, control over intensity, and flexible behavioral responses.
Regarding psychoactive substance use, the patient reported no use during the 2-month treatment and the following 3-month post-treatment phase, confirmed by the DAST-10 (initial 10, final 9). The change in question 3 (Can you stop using drugs when you want?) suggests greater control over substance use.
In summary, the results show improvements in emotional regulation, decreased experiential avoidance, and reduced substance use, though continued intervention and follow-up are still needed.
Discussion
This clinical case study examined the effects of DBT and culturally adapted ACT in Colombia for treating psychoactive substance use, experiential avoidance, and emotional dysregulation. The findings provide valuable insights into third-generation therapies. Dialectical behavior therapy integrates behavioral and dialectical strategies to address emotional dysregulation and promote changes in problematic behaviors (Linehan et al., 1999), while ACT focuses on psychological inflexibility by enhancing acceptance, cognitive defusion, value-based living, and committed action.
The analysis of contextual therapies revealed that early traumatic experiences, such as exposure to violence and substance use within the family, contributed significantly to the development of psychological and behavioral difficulties. Biological and contextual vulnerabilities, including the patient’s father’s criminal behavior and violent upbringing, worsened the emotional and behavioral challenges. These factors were compounded by emotional dysregulation, where heightened sensitivity and intense emotional reactivity further exacerbated the difficulties (Krotter et al., 2024; Linehan et al., 1999).
Adverse childhood experiences (ACEs) were also pivotal in shaping the patient’s struggles in adulthood. These included physical, sexual, and emotional abuse, as well as the traumatic loss of his father, which had a lasting impact (Gallego et al., 2020). Traumatic processing of these events is strongly associated with substance use disorders, emphasizing the need for trauma-informed interventions.
The ASSIST revealed a high risk for opioid and other substance use (see Table 5), emphasizing the necessity of immediate intervention. Despite receiving methadone substitution therapy for heroin addiction, the patient’s emotional distress during the assessment highlighted the need to address emotional dysregulation and psychological inflexibility. A key therapeutic goal was cognitive defusion, which helped the patient detach from distressing thoughts linked to traumatic events, reducing discomfort and emotional dysregulation (Michałowska & Cheć, 2024).
Improvements in experiential avoidance and psychological flexibility were evident through decreased scores on the Acceptance and Action Questionnaire-II (AAQ-II) and the BEAQ, indicating DBT’s effectiveness in promoting emotional acceptance and cognitive flexibility (Ii et al., 2019). The CFQ showed that the patient developed the ability to observe thoughts objectively and distance himself from traumatic memories, reflecting a reduction in cognitive fusion and dysfunctional behaviors (Hayes et al., 2011).
In emotional regulation, the patient demonstrated improvements in managing emotions, evidenced by lower scores on the Difficulties in Emotion Regulation Scale (DERS), which supports the role of DBT in developing emotional regulation skills. Regarding substance use, the patient showed abstinence from psychoactive substances during the 2-month treatment and 3-month follow-up period, which, coupled with increased autonomy in drug use decisions, suggested a shift in attitudes and a reduction in addictive behaviors (Linehan et al., 1999).
The implementation of DBT and ACT strategies significantly improved the patient’s relationship with his internal experiences, enabling him to better manage emotions, thoughts, and situations that previously triggered cravings and substance use. This outcome emphasizes the relevance of integrating third-generation therapies in addressing complex clinical cases involving emotional dysregulation, experiential avoidance, and substance use (Michałowska & Cheć, 2024).
This case study highlights the effectiveness of DBT and ACT in reducing substance use, emotional dysregulation, and experiential avoidance within the Colombian context. Although significant improvements were made, areas such as emotional regulation require continued intervention and interdisciplinary support. The findings underscore the importance of ongoing, individualized therapeutic efforts to address persistent challenges and promote well-being.
In conclusion, this study demonstrates the applicability of culturally adapted DBT and ACT in treating psychoactive substance use and associated psychological challenges. The results reinforce the potential of these therapies as third-generation approaches for addressing complex mental health issues and the necessity of addressing underlying trauma and emotional vulnerabilities through tailored interventions. These findings lay the groundwork for further research and application of DBT and ACT in diverse cultural settings.
Acknowledgements
It is carried out as part of the fulfillment of the requirements for training and graduation in the Doctorate in Psychology of the Universidad Simón Bolívar, Barranquilla, under the modality of Scholarship granted by MINCIENCIAS from the Program of training and insertion of high-level human capital for the regions for the biennium 2021-2022. We acknowledge the support of the publication cost by the Universidad Simón Bolívar, Colombia.
Ethical approval
This study was approved by the Comité de ética de investigación Universidad Simón Bolívar (Date: Junio 29, 2023, Decision/Protocol No: CIE-USB-0478-00). Additionally, written informed consent was obtained from the patient(s) or their legal guardians for the publication of this study and any accompanying images.
Data availability statement
The data supporting the findings of this study are not publicly available due to the clinical nature of this case report and the protection of patient confidentiality.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Axelrod, S. R., Perepletchikova, F., Holtzman, K., & Sinha, R. (2011). Emotion regulation and substance use frequency in women with substance dependence and borderline personality disorder receiving dialectical behavior therapy. American Journal of Drug and Alcohol Abuse, 37(1), 37-42. https://doi.org/10.3109/00952990.2010.535582
- Bohórquez-Borda, D., Gómez-Villarraga, D., Bernal-Cundy, M., Iriarte-Becerra, S., Ramírez-Moreno, V., & Riveros-Munévar, F. (2023). Difficulties in emotion regulation scale (DERS): Evidence of validity and reliability in Colombian samples. Revista de Psicopatologia y Psicologia Clinica, 28(2), 129-138. https://doi.org/10.5944/rppc.36318
- Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H., Riley, D., & CARE Group* (2013). The CARE guidelines: Consensus-based clinical case reporting guideline development. Global Advances in Health and Medicine, 2(5), 38-43. https://doi.org/10.7453/gahmj.2013.008
- Gallego, A., McHugh, L., Villatte, M., & Lappalainen, R. (2020). Examining the relationship between public speaking anxiety, distress tolerance and psychological flexibility. Journal of Contextual Behavioral Science, 16, 128-133. https://doi.org/10.1016/j.jcbs.2020.04.003
- Hayes, S. C., Villatte, M., Levin, M., & Hildebrandt, M. (2011). Open, aware, and active: Contextual approaches as an emerging trend in the behavioral and cognitive therapies. Annual Review of Clinical Psychology, 7, 141-168. https://doi.org/10.1146/annurev-clinpsy-032210-104449
- Ii, T., Sato, H., Watanabe, N., Kondo, M., Masuda, A., Hayes, S. C., & Akechi, T. (2019). Psychological flexibility-based interventions versus first-line psychosocial interventions for substance use disorders: Systematic review and meta-analyses of randomized controlled trials. Journal of Contextual Behavioral Science, 13, 109-120. https://doi.org/10.1016/j.jcbs.2019.07.003
- Krotter, A., Aonso-Diego, G., González-Menéndez, A., González-Roz, A., Secades-Villa, R., & García-Pérez, Á. (2024). Effectiveness of acceptance and commitment therapy for addictive behaviors: A systematic review and meta-analysis. Journal of Contextual Behavioral Science, 32, 100773. https://doi.org/10.1016/j.jcbs.2024.100773
- Linehan, M. M., Schmidt, H., Dimeff, L. A., Craft, J. C., Kanter, J., & Comtois, K. A. (1999). Dialectical behavior therapy for patients with borderline personality disorder and drug-dependence. American Journal on Addictions, 8(4), 279-292. https://doi.org/10.1080/105504999305686
- Michałowska, S. N., & Cheć, M. (2024). Dialectical behavior therapy in the treatment of trauma. Archives of Psychiatry and Psychotherapy, 26(1), 26-32. https://doi.org/10.12740/APP/172133
- Na, E., Lee, K., Jeon, B. H., Jo, C., Kwak, U. H., Jeon, Y., Yang, K., Lee, E. J., & Jeong, J. (2022). Acceptance and commitment therapy for destructive experiential avoidance (ACT-DEA): A feasibility study. International Journal of Environmental Research and Public Health, 19(24), 16434. https://doi.org/10.3390/ijerph192416434
- Pérez Gálvez, B., García Fernández, L., de Vicente Manzanaro, M. P., Oliveras Valenzuela, M. A., & Lahoz Lafuente, M. (2010). Validación Española del drug abuse screening test (DAST-20 y DAST-10). Health and addictions. Salud y Drogas, 10(1), 35-50.
- Ruiz, F. J., Suárez-Falcón, J. C., Cárdenas-Sierra, S., Durán, Y., Guerrero, K., & Riaño-Hernández, D. (2016). Psychometric properties of the acceptance and action questionnaire-II in Colombia. Psychological Record, 66(3), 429-437. https://doi.org/10.1007/s40732-016-0183-2
- Ruiz, F. J., Suárez-Falcón, J. C., Riaño-Hernández, D., & Gillanders, D. (2017). Psychometric properties of the Cognitive Fusion Questionnaire in Colombia. Revista Latinoamericana de Psicología, 49(1), 80-87. https://doi.org/10.1016/j.rlp.2016.09.006
- Sequeda, G., Acosta-López, J. E., Diaz-Camargo, E., Torres-Santos, E.-A., López-Ramírez, V., & Rivera-Porras, D. (2024). Third-generation therapies for the management of psychoactive substance use in young people: Scoping review. Behavioral Sciences, 14(12), 1192. https://doi.org/10.3390/bs14121192
- Shorey, R. C., Gawrysiak, M. J., Elmquist, J., Brem, M., Anderson, S., & Stuart, G. L. (2017). Experiential avoidance, distress tolerance, and substance use cravings among adults in residential treatment for substance use disorders. Journal of Addictive Diseases, 36(3), 151-157. https://doi.org/10.1080/10550887.2017.1302661
- UNODC (2023). Executive summary, World Drug Report. In New Directions for Youth Development, 2012(133). https://www.oecd.org/innovation/inno/47164461.pdf
- Valladolid, G. R., Martínez-Raga, J., Martínez-Gras, I., Alfaro, G. P., Bértolo, J. (2014). Validation of the Spanish version of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Psicothema, 26(2), 180-185. https://doi.org/10.7334/psicothema2013.172
- Vázquez-Morejón, R., León Rubio, J. M., Martín Rodríguez, A., & Vázquez Morejón, A. J. (2019). Validation of a Spanish version of the Brief Experiential Avoidance Questionnaire (BEAQ) in clinical population. Psicothema, 31(3), 335-340. https://doi.org/10.7334/psicothema2019.60
- World Health Organization (2018). Adverse Childhood Experiences International Questionnaire (ACE-IQ). Geneva: World Health Organization. https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-%28ace-iq%29
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.