Abstract
The Exercise Addiction Inventory-3 is the latest version of the Exercise Addiction Inventory, whose use has become more frequent in several countries. The present study investigated its psychometric properties among Turkish adults. The study recruited 389 participants through online social media platforms. Reliability was tested through Cronbach’s alpha and McDonald’s omega. Validity was tested through correlations among the Exercise Addiction Inventory-3 score and scores on the Exercise Dependence Scale-Revised, Ten-Item Personality Inventory, SCOFF Questionnaire, and Obsessive-Compulsive Inventory-Revised. Structural validity was tested via confirmatory factor analysis and measurement invariance. The findings suggested that the Turkish version of the Exercise Addiction Inventory-3 is reliable. Moreover, confirmatory factor analysis indicated that the models demonstrated good to excellent fit indices. Partial measurement invariance was observed. The Exercise Addiction Inventory-3 scores were positively correlated with the Exercise Dependence Scale-Revised and Obsessive-Compulsive Inventory-Revised scores. The total scale score and the Addiction Tendency subscale score were negatively correlated with SCOFF scores but not the Health Relevance subscale scores. The Turkish Exercise Addiction Inventory-3 is a reliable and valid instrument to assess the risk of exercise addiction that differentiates at-risk groups from passionate exercisers. Implications for future studies are discussed.
Keywords: behavioral addiction, confirmatory factor analysis, Exercise Addiction Inventory, psychometric evaluation
Main Points
- The study assessed both the reliability and validity of the Turkish Exercise Addiction inventory-3 (EAI-3).
- The EAI-3 has good psychometric properties, showing reliability and validity for assessing the risk of exercise addiction.
- Confirmatory factor analysis indicates that the models had good to excellent fit indices, with partial measurement invariance observed between female and male exercisers.
- The EAI-3 scores positively correlate with scores on the Exercise Addiction Scale-Revised and Obsessive-Compulsive Inventory-Revised and negatively correlate with scores on the SCOFF Questionnaire.
- The Turkish EAI-3 is a valid tool for assessing exercise addiction and distinguishing at-risk groups from passionate exercisers.
Introduction
Exercise addiction (EA) can be conceptualized as a behavioral addiction that involves a persistent pattern of exercise leading to negative consequences on an individual’s physical (e.g., injuries), psychological, and social well-being (e.g., decreased social interactions; Adams & Kirkby, 2001). Empirical evidence suggests that EA has characteristics of psychological dependence (e.g., withdrawal-like symptoms and cravings) that are experienced in substance addictions as well as in gambling or gaming addictions (Freimuth et al., 2011). However, the Diagnostic and Statistical Manual of Mental Disorders, fifth edition text revision (DSM-5-TR; [xRef no="3"]American Psychiatric Association [APA], 2022[/xRef]), the standard diagnostic text used by mental health professionals, does not yet include exercise addiction as a formal diagnostic category due to insufficient scientific evidence for diagnostic standards and uniformity in etiology (Szabo & Demetrovics, 2022).
One challenge that hinders the establishment of a standardized diagnostic framework is the heterogeneity in EA (Weinstein & Szabo, 2023). Exercise addiction can be classified as primary or secondary. Primary exercise addiction is when the rewarding effects stem directly from exercise behavior, whereas secondary exercise addiction, better conceptualized as instrumental exercise, refers to exaggerated exercise to gain a reward that is not related to exercise, such as weight loss or building a muscular body (Szabo & Demetrovics, 2022). However, as discussed by Colledge et al. (2020), sometimes the difference between the types of exercise addiction or the frequency of diagnosis can be biased. In fact, some studies either fail to assess the prevalence of eating disorders among individuals engaging in excessive exercise or deliberately exclude participants with eating disorder symptoms to focus solely on those meeting the criteria for primary exercise addiction.
The other difficulty in EA research is that engaging in high levels of exercise is a combination of commitment and passion, which blurs the line between healthy and unhealthy (Szabo, 2018). The detection of such a threshold is mandatory in the diagnostic phase. Therefore, it is crucial to develop a scale that is accurate and valid for assessing exercise addiction so that researchers and clinicians can identify individuals not only “at risk” but also screen those suffering from exercise-related dysfunction (Granziol et al., 2023).
During the past few decades, various instruments have been developed. Two of the most widely used are the Exercise Dependence Scale (EDS-R; Hausenblas & Downs, 2002) and the Exercise Addiction Inventory (EAI; Terry et al., 2004). Recently, an expanded EAI version (EAI-3; Granziol et al., 2023) was developed to assess exercise addiction more sensitively.
In their comparative study of the psychometric characteristics of the EDS-R and EAI, Mónok et al. (2012) noted that both instruments are reliable and sensitive enough to assess and differentiate addiction levels among exercisers, with interesting commonalities in the assessed symptoms (e.g., tolerance, withdrawal, and modification; Gauld et al., 2023). In recent years, the EAI has also been revised to assess more aspects of EA. Granziol et al. (2023) proposed a new version (i.e., EAI-3) investigating aspects such as feelings of guilt accompanied by exercise addiction and the tendency to exercise regardless of injury, perhaps not following medical advice. The EAI-3 has several advantages: a more straightforward classification (i.e., being at risk or not), as determined by the total score; and a two-factor structure (i.e., Addiction Tendency and Health Relevance subscales), helping the user to consider both pathological and healthy/passion-related sides of exercise (Granziol et al., 2023).
Although the EAI-3 has been validated in several languages, neither its reliability nor its validity have been formally evaluated among Turkish samples. Therefore, the present study addressed this research gap. Firstly, good psychometric properties in terms of the Turkish EAI-3’s reliability and validity (H1) were expected. Moreover, it was also hypothesized that the Turkish EAI-3 would have a two-factor structure (H2), that the scale would demonstrate measurement invariance between female and male exercisers (H3), and that the previously established cutoff score (i.e., 34) suggesting the risk of exercise addiction would be found among Turkish adults (H4).
Material and Methods
Participants
Individuals aged 18 years and over who exercised for an average of 150 minutes at least three days per week and had maintained regular physical activity for at least six months were eligible to be included in the study. These criteria, which are coherent and in line with the World Health Organization’s (2020) definition of regular exercisers, were used to include all the exercises that regular exercisers did or trained themselves in sports or physical activity. This definition has also been used in prior studies (e.g., Huang et al., 2019) and excludes individuals who do not regularly exercise or whose training/exercise rate is not enough to make them prone to exercise addiction. The exclusion criteria were being aged below 18 years, not exercising at least three times weekly, not exercising for at least 150 minutes per session, and not exercising regularly for at least six months.
Measures
Demographic Information
The initial sample comprised 449 participants. The final sample comprised 389 participants (60.15% male; Mage = 27.12 years; SD = ±8.81; age range = 18-56 years; age data missing for 41 participants). The sample comprised 155 female participants (39.89%) and 234 male participants (60.15%). More demographic information can be found in the Supplementary Material.
Expanded Exercise Addiction Inventory
The EAI-3 is an eight-item questionnaire (e.g., “Concerns have arisen between me and my family and/or my partner about the amount of exercise I do”). Items are rated on a six-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). The EAI-3 includes the Health Relevance (HR) and Addiction Tendency (AT) subscales (Granziol et al., 2023). Total scores range from 8 to 54. Adaptation to the Turkish language was conducted according to the standard translation-back translation procedure (Beaton et al., 2000). All the items and their assignment to each subscale are in the Appendix.
Exercise Dependence Scale-Revised
The EDS-R (Hausenblas & Downs, 2002; Turkish version: Yeltepe & İkizler, 2007) comprises 21 items and seven sub-dimensions. The items were based on DSM-IV substance addiction criteria. Each item (e.g., “I continually increase my exercise intensity to achieve the desired effect/benefits”) is scored on a six-point Likert scale, ranging from 1 (never) to 6 (always). The total scores range from 21 to 126. Higher scores indicate a greater risk of exercise dependence.
The SCOFF Questionnaire
The five-item SCOFF (sick, control, one stone, fat, and food) Questionnaire (Morgan et al., 1999; Turkish version: Aydemir et al., 2015) was used to assess the risk of developing an eating disorder. Each item (e.g., “Do you make yourself sick because you feel uncomfortably full?”) is answered either “yes” or “no” (a “yes” scores 1-point). Scores greater than 2 (out of 5) suggest a positive screening for a potential eating disorder.
Obsessive-Compulsive Inventory-Revised
The OCI-R (Abramowitz & Deacon, 2006; Yorulmaz et al., 2015) was used to assess obsessive and compulsive symptoms. The inventory comprises 18 items and 6 subscales evaluating washing, checking, ordering, obsessing, hoarding, and neutralizing symptoms. Each item (e.g., “I am upset by unpleasant thoughts that come into my mind against my will”) is scored on a five-point scale from 0 (not at all) to 4 (extremely). The range of the total score is 0-72, with higher scores suggesting more severe OCD symptoms.
Ten-Item Personality Inventory
The Ten-item Personality Inventory (TIPI) (Gosling et al., 2003; Turkish version: Atak, 2013) was used to assess five personality traits, namely extraversion, conscientiousness, agreeableness, openness to experience, and emotional stability (two items for each trait). Each item (e.g., “I see myself open to new experiences, complex”) is scored on a seven-point scale from 1 (disagree strongly) to 7 (agree strongly). The psychometric properties of all the scales (excluding EAI-3) are in the supplementary materials.
Procedure
Data were collected through an online survey disseminated via social media platforms. More specifically, recruitment posts were shared on Facebook, Instagram, and Twitter. The recruitment strategy targeted public and private groups, pages, and forums with a clear affiliation to sports, fitness, and exercise-related interests (e.g., amateur sports teams, fitness communities, and exercise science discussion groups). These groups were selected based on their thematic relevance and high likelihood of participation from individuals who regularly engage in physical activity. To enhance sample diversity and increase participation, a snowball sampling approach was also implemented. Upon completing the survey, participants were invited to share the survey link with acquaintances or peers who also engaged in regular exercise. This strategy aimed at reaching a broader population of exercisers beyond the initial distribution channels.
The survey was conducted on the Qualtrics research platform. After obtaining written consent, the participants were informed about the general study idea. Participants were free to quit the study at any point. They were informed that their data would be processed anonymously. Participants were not paid or rewarded in any way for their participation. The study received ethics committee approval (University of Padova, code: 18F7D86802A124B1E783A3074ED80641).
Data Analysis
Because the structure of the EAI-3 was previously identified by Granziol et al. (2023), only a confirmatory approach (i.e., CFA) was used. Moreover, measurement invariance based on biological sex, reliability, and validity analyses were performed. The R statistical software was used to run all analyses and the lavaan package for the CFA models.
Confirmatory Factor Analysis and Measurement Invariance
To obtain more robust results, standard errors, and mean adjusted test statistics, a robust version of the maximum likelihood estimator method was used. The model’s fit was assessed through the comparative fit index (CFI: estimates ≥0.95 for a good fit, estimates ≥0.90 for an adequate fit, while estimates <0.90 suggesting a non-acceptable fit); and the root mean square error of approximation (RMSEA: estimates ≤0.05 indicate a good fit, estimates between 0.05 and 0.10 an adequate fit, and estimates >0.10 a non-acceptable fit).
Measurement invariance (MI in the sequel) of the item scores was tested to understand whether biological sex might influence the participants’ responses. As a first step, a baseline model was tested to examine the fundamental structure of the EAI-3. Then, configural, metric, and scalar models were tested. Both the difference (Δ) between fit indices of the models (CFI > 0.01 and an RMSEA > 0.015 indicated invariance violations) and the overall fit of each model were used as criteria to assess MI. Partial measurement invariance was tested whenever MI violations emerged by relaxing only the parameters related to the critical item(s).
Reliability, Validity and Cutoff, and Linear Models
Cronbach’s alpha and McDonald’s omega indices were used to evaluate reliability and internal consistency. For both indices, a value ≥0.70 suggests good reliability. The receiver operating characteristic (ROC) curve was adopted to assess both specificity and sensitivity of EAI-R. The EDS-R categorical score was used as a criterion to define the best EAI-3 cutoff. Both concurrent and convergent validity were assessed by using the Spearman correlation coefficient of both total scale and subscale scores with all the scales and subscale scores of the EDS-R OCI-R, SCOFF, and TIPI. All p-values were adjusted through a false discovery rate correction.
Finally, to check if other sample characteristics may relate to the risk of exercise addiction, three linear regression models were tested, with the EAI-3 total score as the response variable and three different predictors: the type of exercise (three levels: aerobic, anaerobic or both; model 1), type of exercise participation (three levels: individual, team or both; model 2), and purpose of exercise (physical/mental health, mastery or social; model 3). Because the frequencies of the predictors’ levels may be very different, two precautions were adopted. First, a priori comparisons by using Helmert contrasts were used on each categorical variable. Helmert contrasts belong to a family of centered and orthogonal contrasts coding, where each level of a categorical variable is tested against the means of all the previous ones. With Helmert contrasts (and due to the orthogonality, see Granziol et al. (2025)) each comparison can be interpreted independently of the others. Therefore, it is possible to compare the levels with similar frequencies (first comparison), as well as the mean of the levels with similar frequencies with the mean of levels with the highest or the lowest frequencies. Secondly, the homoscedasticity of each model was tested before commenting on the results, using Levene’s test. Whenever the assumption of homoscedasticity was violated, the model was not commented on.
Results
Confirmatory Factor Analysis and Measurement Invariance
From Table 1, it can be observed that all the CFA models (overall and MI) obtained good to excellent fit indices. Configural and metric invariance emerged, as suggested by the adequate fit indices. However, scalar invariance violations were observed. As suggested by modifications indices inspections, the intercept on Item 2 (“Concerns have arisen between me and my family and/or my partner about the amount of exercise I do”; MI = 19.278) was different between females and males. Males presented higher starting values on this item (M = 2.68; F = 1.94). Relaxing parameters related to this item led to an improvement of the model, but further scalar violation was found on Item 8 (“I am inclined to train when [or before completely recovered from] illness or injury”; MI = 8.214). More specifically, males had higher starting values on this item (M = 3.76; F = 3.16). Even in this case, item parameters relaxation led to a model improvement, but further scalar violation was found on Item 1 (“Exercise is the most important thing in my life”; MI = 6.172). More specifically, males had higher starting values on this item (M = 4.32; F = 4.02). Relaxing parameters related to this item improved model fit, and no further violations were found.
|
Results of the CFA on the assessment model comprising eight items. Note: CFI = Comparative fit Iidex; RMSEA = Root mean square error of approximation; Δ = Difference; I2 = Invariance on item 2, I28 = Invariance on items 2 and 8; I128 = Invariance on items 1, 2, 8. |
||||
| Table 1. Results of the confirmatory factor analysis on the assessment model composed of eight items | ||||
| Model |
|
|
|
|
| Overall |
|
|
|
|
| TR-female |
|
|
|
|
| TR-male |
|
|
|
|
| Configural |
|
|
|
|
| Metric |
|
|
|
|
| Scalar |
|
|
|
|
| Scalar I2 |
|
|
|
|
| Scalar I28 |
|
|
|
|
| Scalar I128 |
|
|
|
|
Reliability
The EAI-3 overall scale scores obtained good internal consistency (Cronbach’s α = 0.81; McDonald’s ω = 0.85). Both HR (Cronbach’s α = 0.74; McDonald’s ω = 0.76) and AT subscales (Cronbach’s α = 0.71; McDonald’s ω = 0.78) had acceptable internal consistency.
Exercise Addiction Inventory-3 Cutoffs
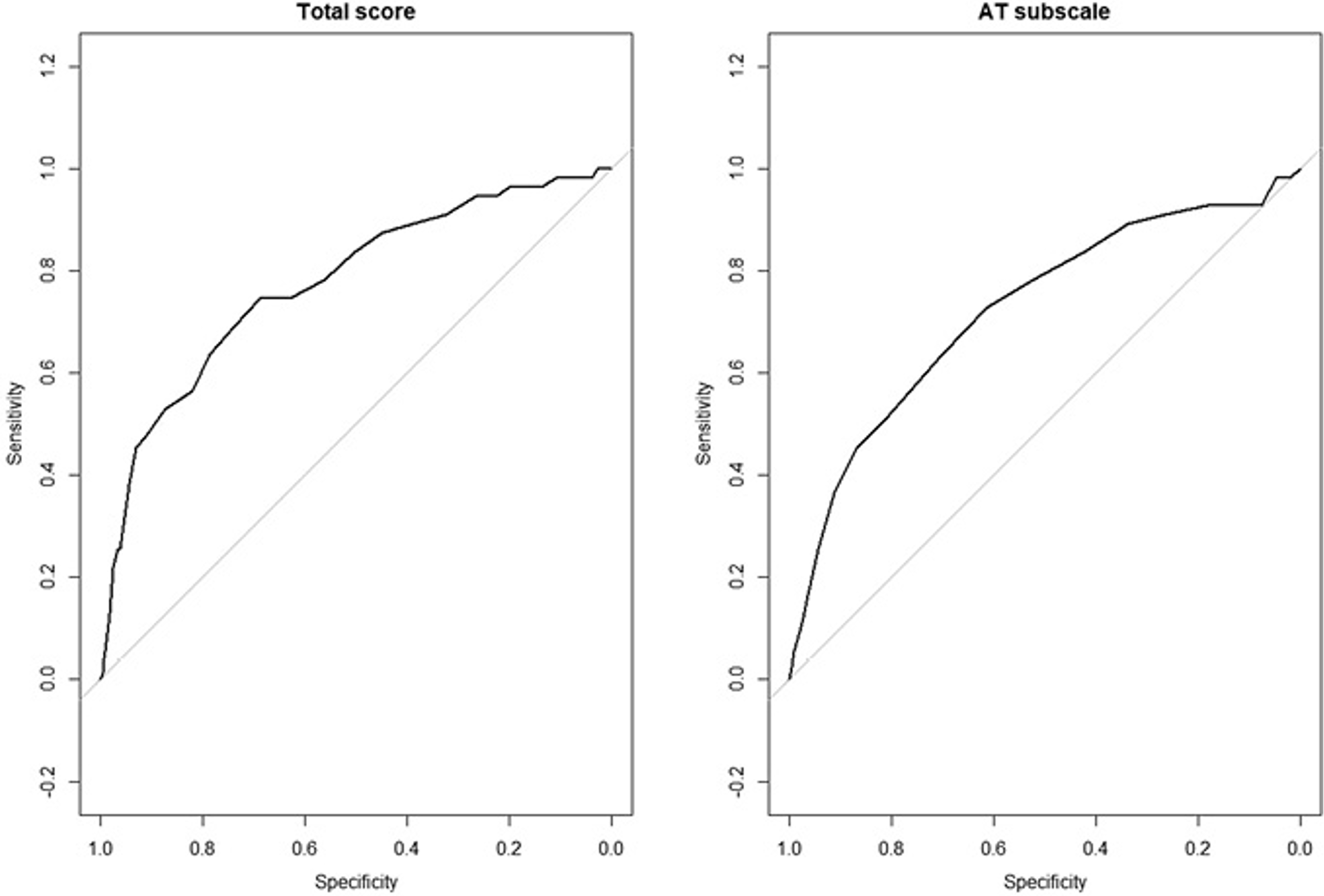
Applying the EDS-R cutoff, 55 participants (14 F, 41 M) were identified as at risk of developing exercise addiction, while 334 participants (141 F, 193 M) were identified as not at risk. Based on this, ROC analysis suggested that a cutoff of 32.5 for the total score of the EAI-3 was sufficient to suggest a potential risk of exercise addiction (specificity: 0.688; sensitivity: 0.745; AUC: 0.774; see Figure 1, left panel). In regard to the AT subscale, a cutoff of 14.5 could be used to suggest an at-risk state (specificity: 0.613; sensitivity: 0.727; AUC: 0.722; Figure 1, right panel). Starting from this cutoff (i.e., considering total score), 55 respondents were screened as at risk of exercise addiction (14.13%).
Concurrent Validity, Convergent Validity, and Linear Models
Both total and subscale scores showed moderate to high correlation with EDS-R, suggesting adequate criterion validity. Positive correlations between EAI-3 scores and both SCOFF and OCI total scores (excluding HR subscales in the former case) were found, with AT scores having (in absolute value) a higher correlation with such scales. The HR subscale scores were positively correlated with agreeableness, conscientiousness, and openness scores on the TIPI. Finally, the total EAI-3 score was positively associated with the openness score on the TIPI (see Table 2). No further statistically significant correlations were found.
|
Bonferroni adjustment method was used. Note: ρ = Spearman’s correlation coefficient; p adj = Adjusted p-value; AT = Addiction tendency subscale; EAI = Exercise addiction scale; EDSR = Exercise dependence scale-revised; HR = Healthy relevance subscale; OCIR = Obsessive-compulsive inventory-revised; SCOFF = SCOFF Questionnaire. |
|||
| Table 2. The correlations between the eai-3 scores and scores on the other scales | |||
| EAI-3 | Other Scales |
|
|
| EDSR_tot | HR |
|
|
| EDSR_tot | AT |
|
|
| EDSR_tot | EAI_tot |
|
|
| HR | OCIR_tot |
|
|
| AT | OCIR_tot |
|
|
| EAI_tot | OCIR_tot |
|
|
| HR | SCOFF |
|
|
| AT | SCOFF |
|
|
| EAI_tot | SCOFF |
|
|
| HR | Extraversion |
|
|
| AT | Extraversion |
|
|
| EAI_tot | Extraversion |
|
|
| HR | Agreeableness |
|
|
| AT | Agreeableness |
|
|
| EAI_tot | Agreeableness |
|
|
| HR | Consciousness |
|
|
| AT | Consciousness |
|
|
| EAI_tot | Consciousness |
|
|
| HR | Emotional stability |
|
|
| AT | Emotional stability |
|
|
| EAI_tot | Emotional stability |
|
|
| HR | Openness |
|
|
| AT | Openness |
|
|
| EAI_tot | Openness |
|
|
In the linear model, Table 3 shows the descriptive statistics on the three predictors used for the three linear models: the exercise type (three levels: aerobic, anaerobic or both; model 1), type of exercise participation (three levels: individual, team or both; model 2), and purpose of exercise (physical/mental health, mastery or social; model 3). The difference in frequencies for at least one level in each variable was coherent with the analytic plan.
| Note: Max = Maximum; Min = Minimum; SD = Standard Deviation. | |||||||
| Table 3. Descriptive statistics of the categorical variables as predictors of the linear models on eai total scores | |||||||
| Characteristic | Level |
|
|
|
|
|
|
| Sport type | Aerobic |
|
|
|
|
|
|
| Sport type | Anaerobic |
|
|
|
|
|
|
| Sport type | Mixed |
|
|
|
|
|
|
| Individial/team | Individual |
|
|
|
|
|
|
| Individial/team | Team |
|
|
|
|
|
|
| Individial/team | Both |
|
|
|
|
|
|
| Purpose | Health |
|
|
|
|
|
|
| Purpose | Mastery |
|
|
|
|
|
|
| Purpose | Social |
|
|
|
|
|
|
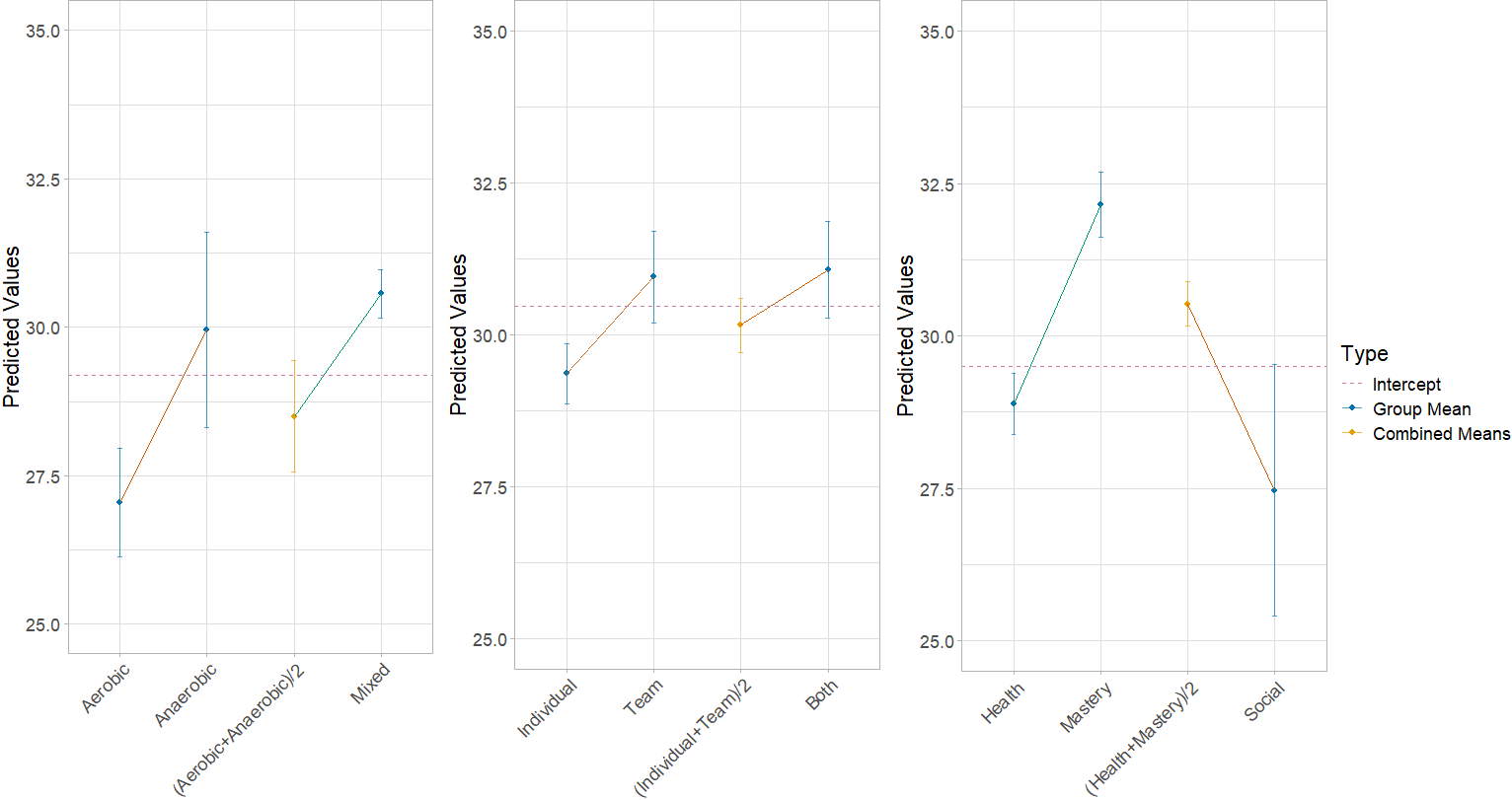
Levene’s test did not show any significant deviations from homoscedasticity (model 1: F (2, 386) = 0.88, p = .41; model 2: F (2, 386) = 0.09, p = .91; model 3: F (2, 386) = 1.78, p = .17). In model 1, no differences were found comparing participants engaging in anaerobic vs. aerobic sport (b = 1.45; SE = 0.95, t = 1.53, p = .13). However, when comparing the average EAI-3 score of participants engaging in aerobic or anaerobic sports separately with the average EAI-3 score of participants engaging in both, the latter means emerged as significantly higher than the former (b = 0.69; SE = 0.34, t = 2, p = .04; left panel of Figure 2). In model 2, no differences were found in both comparisons (comparison 1: b = 0.79; SE = 0.40, t = 1.81, p = .07; comparison 2: b = 0.31; SE = 0.32, t = 0.98, p = .32; middle panel of Figure 2). Finally, in model 3, participants exercising for mastery purposes obtained higher average values of EAI-3 total scores compared to participants exercising for health purposes (b = 1.63; SE = 0.37, t = 4.37, p < .01; right panel of Figure 2), while no differences were found comparing participants exercising for social purposes to participants exercising for health and mastery purposes together (b = −1.01; SE = 0.62, t = −1.63, p = .10).
Discussion
Because its definition and assessment are still developing, exercise addiction is not yet formally recognized as a mental health disorder. Numerous scales are available that assess problematic exercise, and these have been validated in multiple languages. The Turkish EAI was only recently validated (Aydın et al., 2023). Since then, the EAI-3 has been developed, and the present study investigated both the reliability and validity of the EAI-3 among Turkish adults, and the results showed it had good psychometric properties (supporting H1). The overall reliability analysis of the Turkish EAI-3 indicated adequate to very good reliability for both the overall scale and its two subscales.
In addition, the internal consistency coefficients obtained in the analysis align with those reported in Granziol et al.’s (2023) original validation study, where the total scale demonstrated adequate internal consistency (α = 0.81; ω = 0.84). An acceptable internal consistency was found for both the HR subscale (α = 0.70; ω = 0.74) and the AT subscale (α = 0.71; ω = 0.78). The second hypothesis concerned the two-factor structure of the EAI-3. The confirmatory factor analysis (CFA) confirmed the two-factor structure of the EAI-3 among Turkish individuals (supporting H2), with one factor assessing HR and the other assessing AT. One of the main challenges that remains is distinguishing healthy, passionate physical activity from exercise addiction when both addicted and passionate participants use the scale. Differentiating between passionate and addicted individuals would allow for the EAI-3’s further use in clinical screening and better identification of people truly at risk of EA, thereby reducing the possibility of false positives.
In the present study, violations of scalar invariance were observed for EAI-3 Item 1 (“Exercise is the most important thing in my life”), Item 2, (“Concerns arose between me and my family and/or partner about the amount of exercise I do”), and item 8 (“I am inclined to train when (or before completely recovering from illness or injury”), indicating a lack of invariance in the item responses across gender (initially not supporting H3). The violation indicated that the intercepts differed between males and females for all items listed, with males having higher starting values than females. After the parameters were relaxed, measurement invariance across gender was established, indicating that the scale performed equally well for both male and female participants among Turkish individuals (supporting H3). These potential differences between Turkish males and females can be interpreted from several perspectives.
First, Item 1 may reflect the commitment of Turkish males to sports. However, on a broader scale, family plays a central role in Turkish culture, and females are generally expected to take on more and various responsibilities within the family than males. Despite having the same level of commitment to sports, Turkish females may feel more societal pressure to prioritize family and/or their partners, leading them to score lower on Item 1 than their male counterparts. Furthermore, Item 1 of the EAI-3 was also associated with measurement invariance in the original study (Granziol et al., 2023). This might indicate that the content of Item 1 is not ideal for capturing the salience component of exercise addiction.
Secondly, for Item 2, the difference observed between females and males could be explained by the fact that males generally have higher physical endurance than females and, therefore, can exercise more frequently, which might influence the amount of time spent exercising (Högström et al., 2012). Additionally, it should be noted that among the general Turkish population, the level of physical activity is generally lower among females than males (Daşkapan & Atalay, 2013).
Lastly, for Item 8, in Turkish culture, gender stereotypes suggest that males should be strong, ambitious, and brave (Sakallı & Kuzlak, 2018). Consequently, males might challenge themselves more to fulfill these stereotypes than their female counterparts, leading them to return to exercising before fully recovering or to exercise while still injured.
The last hypothesis of the present study (H4) was that the internationally recognized cutoff score of the EAI-3 (i.e., a total score of 34) would be expected to have a good fit for the Turkish data. However, the results of this study did not support this hypothesis. Instead, the results of the study determined a Turkish cutoff score one point lower than the original study (Granziol et al., 2023). This indicates that the psychometric properties of the Turkish EAI-3 may differ slightly from the original version. The sensitivity value in the present study might be related to the sample’s demographics, such as age, which was not controlled for. Therefore, studies with larger numbers of participants are needed to achieve more consistent results. Because exercise addiction is still an evolving field of research, a cross-culturally comparable cutoff score can play a pivotal role in solidifying the foundation of exercise addiction and its potential diagnostic properties in the future.
Regarding the relationship between the EAI-3 and other scales, the EAI-3 indicated concurrent validity with the EDS-R, indicating that the EAI-3 appears to capture the same construct as the EDS-R and therefore has good concurrent validity. Additionally, a positive correlation was observed between AT, one of the two factors of the EAI-3, and the SCOFF. Unlike the original study (Granziol et al., 2023), no correlation was found between the HR factor and SCOFF. This may suggest that when sport and exercise are perceived through their impact on health or as elevated passion, the relationship with the risk of eating disorders is difficult to identify. However, the relationship between the total EAI-3 score and its pathological scale scores and the SCOFF showed a significant positive correlation, consistent with the established relationship between exercise addiction and eating disorders in the literature (Shroff et al., 2006; Cook et al., 2015). Trott et al. (2021) reported in their meta-analysis that exercise addiction occurs more frequently among individuals with eating disorders than those without. Similarly, Zeulner et al. (2016) found that 44.4% of participants who scored positively on the EAI were also at risk for developing an eating disorder.
Another result from the present study was that the EAI-3 and its subscales did not correlate with neuroticism, which is defined as emotional instability and heightened stress response resulting in frequent negative emotions. This result contradicts the study by Remilly et al. (2023), in which participants reported higher levels of neuroticism correlated with higher EDS-R scores, whereas Costa and Oliva (2012) found that emotional (in)stability (neuroticism) negatively correlated with exercise addiction. This discrepancy may stem from differences in instruments and sample characteristics between studies. It may also suggest that the EAI-3 captures different profiles and patterns of exercise addiction.
Scores on one of the subscales of the EAI-3, AT, were positively correlated with scores on the Obsessive-Compulsive Inventory-Revised (OCI-R). Gulker et al. (2001) reported that excessive exercisers exhibited higher rates of obsessive-compulsive symptoms, such as an association between eating disorders and obsessive-compulsive traits (Lichtenstein et al., 2017). This is consistent with the correlation observed between the pathological factor in the factorial structure of the EAI-3 and the OCI-R in the present study. Additionally, in the study by Meyer et al. (2021), 31.3% of individuals with exercise addiction had obsessive-compulsive disorders, and 25% of individuals had obsessive-compulsive personality disorder. This comorbidity with several other diagnoses supports the idea that exercise addiction is a separate construct from eating disorders, but somehow related to other disorders. Based on this, obsessive-compulsive spectrum disorders and behavioral addictions may be important because of their strong emphasis on problematic and repetitive behaviors (Starcevic, 2016).
Finally, interesting results emerged from linear models on EAI-3 total scores and type of exercise engaged in, suggesting that individuals engaged in mixed sports (i.e., aerobic and anaerobic) may be more prone to the risk of exercise addiction than individuals engaging in aerobic or anaerobic activities separately, as suggested by higher total scores in the former group. This may be explained by considering the amount of exercise and time necessary to engage simultaneously in both anaerobic and aerobic sports, factors that may increase the chance of converting a passion into an addiction. Results of the present study also suggested that individuals exercising to master sports at higher levels may be at greater risk of exercise addiction compared to individuals exercising for physical or mental health purposes. These results are in line with studies investigating the edge between passion for exercise and exercise addiction (Szabo & Kovacsik, 2019).
Limitations and Future Research
Some limitations should be mentioned. Data were collected through online self-report measures, which may limit control over the data collection process due to variations in participants’ environments, such as interruptions during the test, potentially affecting response times, and the inability to resolve possible misunderstandings about the questions. Specific exclusion criteria were applied to the data collected. For example, removing participants with a survey completion time lower than seven minutes on average is thought to help improve the overall quality of the data. Moreover, the test-retest reliability of the Turkish version of the EAI-3 was not explicitly assessed. Future research should evaluate the temporal reliability of the EAI-3 to ensure consistency over time.
Thirdly, the present study did not examine the impact of age, prior exercise experience, or the impact of other sample characteristics (such as type of practiced sport or main reason for exercising) on measurement invariance. Although some of these characteristics were used in preliminary linear models that led to interesting results, the difference in category frequencies prevented the use of such variables in measurement invariance models. Future studies could provide greater insight regarding measurement invariance by considering these characteristics. A future study could address the limitations above and examine the utility of the EAI-3 to better understand its properties and its relationship to eating disorders, including primary and secondary exercise addiction. Finally, further research could explore what kind of information can be obtained from using the EAI-3 by integrating a clinical qualitative approach into the research process.
In conclusion, the psychometric properties of the Turkish version of the EAI-3 suggest that (and in line with previous results in other countries) this instrument is a reliable and valid tool for identifying individuals at risk of exercise addiction and distinguishing them from highly engaged but non-addicted exercisers.
Ethical approval
This study was approved by the Research Ethics Board of the University of Padova (Date: December, 12, 2021, Decision/Protocol No: 18F7D86802A124B1E783A3074ED80641). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Abramowitz, J. S., & Deacon, B. J. (2006). Psychometric properties and construct validity of the obsessive-compulsive inventory--revised: Replication and extension with a clinical sample. Journal of Anxiety Disorders, 20(8), 1016-1035. https://doi.org/10.1016/j.janxdis.2006.03.001
- Adams, J., & Kirkby, R. (2001). Exercise dependence and overtraining: The physiological and psychological consequences of excessive exercise. Sports Medicine, Training and Rehabilitation, 10(3), 199-222. https://doi.org/10.1080/10578310210395
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425787
- Atak, H. (2013). The Turkish adaptation of the ten-item personality inventory. Noro Psikiyatri Arsivi, 50(4), 312-319. https://doi.org/10.4274/npa.y6128
- Aydemir, Ö., Köksal, B., Yalın-Sapmaz, Ş., & Yüceyar, H. (2015). Kadın üniversite öğrencilerinde REZZY yeme bozuklukları ölçeği Türkçe formunun güvenilirlik ve geçerliliği. Anadolu Psikiyatri Dergisi, 16, 31-35. https://doi.org/10.5455/apd.174219
- Aydın, D., Baltaci, U. B., Erzen, E., Szabo, A., & Griffiths, M. D. (2023). The Turkish version of the exercise addiction inventory: Validity and reliability. ADDICTA: The Turkish Journal on Addictions, 10(2), 184-193. https://doi.org/10.5152/ADDICTA.2023.22077
- Beaton, D. E., Bombardier, C., Guillemin, F., & Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24), 3186-3191. https://doi.org/10.1097/00007632-200012150-00014
- Colledge, F., Sattler, I., Schilling, H., Gerber, M., Pühse, U., & Walter, M. (2020). Mental disorders in individuals at risk for exercise addiction - a systematic review. Addictive Behaviors Reports, 12, 100314. https://doi.org/10.1016/j.abrep.2020.100314
- Cook, B., Hausenblas, H., Crosby, R. D., Cao, L., & Wonderlich, S. A. (2015). Exercise dependence as a mediator of the exercise and eating disorders relationship: A pilot study. Eating Behaviors, 16, 9-12. https://doi.org/10.1016/j.eatbeh.2014.10.012
- Costa, S., & Oliva, P. (2012). Examining relationship between personality characteristics and exercise dependence. Review of Psychology, 19(1), 5-11. https://hrcak.srce.hr/91383.
- Daşkapan, A., & Atalay, K. D. (2013). Perceived exercise benefits and barriers among Turkish women: A pilot study. Fizyoterapi Rehabilitasyon, 24(1), 127-134.
- Freimuth, M., Moniz, S., & Kim, S. R. (2011). Clarifying exercise addiction: Differential diagnosis, co-occurring disorders, and phases of addiction. International Journal of Environmental Research and Public Health, 8(10), 4069-4081. https://doi.org/10.3390/ijerph8104069
- Gauld, C., Francou, C., Millet, G. Y., Kern, L., & Gergelé, L. (2023). A symptom network analysis of exercise addiction and personality on ultra-marathon runners with serious complications. International Journal of Sport and Exercise Psychology, 22(7), 1625-1639. https://doi.org/10.1080/1612197X.2023.2204878
- Gosling, S. D., Rentfrow, P. J., & Swann, W. B., Jr. (2003). A very brief measure of the big-five personality domains. Journal of Research in Personality, 37(6), 504-528. https://doi.org/10.1016/S0092-6566(03)00046-1
- Granziol, U., Griffiths, M. D., Zou, L., Yang, P., Herschel, H. K., Junker, A., Akimoto, T., Stoll, O., Alpay, M., Aydın, Z., Zandonai, T., Di Lodovico, L., Lichtenstein, M. B., Trott, M., Portman, R. M., Schipfer, M., Cook, B., Cerea, S., Egorov, A. Y., … Szabo, A. (2023). The expanded exercise addiction inventory (EAI-3): Towards reliable and international screening of exercise-related dysfunction. International Journal of Mental Health and Addiction, 22(6), 3559-3585. https://doi.org/10.1007/s11469-023-01066-2
- Granziol, U., Rabe, M., Gallucci, M., Spoto, A., & Vidotto, G. (2025). Not another post hoc paper: A new look at contrast analysis and planned comparisons. Advances in Methods and Practices in Psychological Science, 8(1). https://doi.org/10.1177/25152459241293110
- Gulker, M. G., Laskis, T. A., & Kuba, S. A. (2001). Do excessive exercisers have a higher rate of obsessive compulsive symptomatology? Psychology, Health and Medicine, 6(4), 387-398. https://doi.org/10.1080/13548500120087024
- Hausenblas, H. A., & Downs, D. S. (2002). How much is too much? The development and validation of the exercise dependence scale. Psychology and Health, 17(4), 387-404. https://doi.org/10.1080/0887044022000004894
- Högström, G. M., Pietilä, T., Nordström, P., & Nordström, A. (2012). Body composition and performance: Influence of sport and gender among adolescents. Journal of Strength and Conditioning Research, 26(7), 1799-1804. https://doi.org/10.1519/JSC.0b013e318237e8da
- Huang, Q. I. N., Huang, J., Chen, Y., Lin, D., Xu, S., Wei, J., Qi, C., & Xu, X. (2019). Overactivation of the reward system and deficient inhibition in exercise addiction. Medicine and Science in Sports and Exercise, 51(9), 1918-1927. https://doi.org/10.1249/MSS.0000000000001988
- Lichtenstein, M. B., Hinze, C. J., Emborg, B., Thomsen, F., & Hemmingsen, S. D. (2017). Compulsive exercise: Links, risks and challenges faced. Psychology Research and Behavior Management, 10, 85-95. https://doi.org/10.2147/PRBM.S113093
- Meyer, M., Sattler, I., Schilling, H., Lang, U. E., Schmidt, A., Colledge, F., & Walter, M. (2021). Mental disorders in individuals with exercise addiction-A cross-sectional study. Frontiers in Psychiatry, 12, 751550. https://doi.org/10.3389/fpsyt.2021.751550
- Mónok, K., Berczik, K., Urbán, R., Szabo, A., Griffiths, M. D., Farkas, J., Magi, A., Eisinger, A., Kurimay, T., Kökönyei, G., Kun, B., Paksi, B., & Demetrovics, Z. (2012). Psychometric properties and concurrent validity of two exercise addiction measures: A population wide study. Psychology of Sport and Exercise, 13(6), 739-746. https://doi.org/10.1016/j.psychsport.2012.06.003
- Morgan, J. F., Reid, F., & Lacey, J. H. (1999). The SCOFF questionnaire: Assessment of a new screening tool for eating disorders. BMJ, 319(7223), 1467-1468. https://doi.org/10.1136/bmj.319.7223.1467
- Remilly, M., Mauvieux, B., & Drigny, J. (2023). Personality traits associated with the risk of exercise dependence in ultraendurance athletes: A cross-sectional study. International Journal of Environmental Research and Public Health, 20(2), 1042. https://doi.org/10.3390/ijerph20021042
- Sakallı, N., & Kuzlak, A. (2018). How are women and men perceived? Structure of gender stereotypes in contemporary Turkey. Nesne Psikoloji Dergisi, 309-336. https://hdl.handle.net/11511/37903.
- Shroff, H., Reba, L., Thornton, L. M., Tozzi, F., Klump, K. L., Berrettini, W. H., Brandt, H., Crawford, S., Crow, S., Fichter, M. M., Goldman, D., Halmi, K. A., Johnson, C., Kaplan, A. S., Keel, P., LaVia, M., Mitchell, J., Rotondo, A., Strober, M., … Bulik, C. M. (2006). Features associated with excessive exercise in women with eating disorders. International Journal of Eating Disorders, 39(6), 454-461. https://doi.org/10.1002/eat.20247
- Starcevic, V. (2016). Behavioural addictions: A challenge for psychopathology and psychiatric nosology. Australian and New Zealand Journal of Psychiatry, 50(8), 721-725. https://doi.org/10.1177/0004867416654009
- Szabo, A. (2018). Addiction, passion, or confusion? New theoretical insights on exercise addiction research from the case study of a female body builder. Europe’s Journal of Psychology, 14(2), 296-316. https://doi.org/10.5964/ejop.v14i2.1545
- Szabo, A., & Demetrovics, Z. (2022). Passion and addiction in sports and exercise. Routledge. https://doi.org/10.4324/9781003173595
- Szabo, A., & Kovacsik, R. (2019). When passion appears, exercise addiction disappears. Swiss Journal of Psychology, 78(3-4), 137-142. https://doi.org/10.1024/1421-0185/a000228
- Terry, A., Szabo, A., & Griffiths, M. (2004). The Exercise Addiction Inventory: A new brief screening tool. Addiction Research and Theory, 12(5), 489-499. https://doi.org/10.1080/16066350310001637363
- Trott, M., Jackson, S. E., Firth, J., Jacob, L., Grabovac, I., Mistry, A., Stubbs, B., & Smith, L. (2021). A comparative meta-analysis of the prevalence of exercise addiction in adults with and without indicated eating disorders. Eating and Weight Disorders: EWD, 26(1), 37-46. https://doi.org/10.1007/s40519-019-00842-1
- Weinstein, A. M., & Szabo, A. (2023). Exercise addiction: A narrative overview of research issues. Dialogues in Clinical Neuroscience, 25(1), 1-13. https://doi.org/10.1080/19585969.2023.2164841
- World Health Organization. (2020). WHO guidelines on physical activity and sedentary behaviour. https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf?sequence=1&isAllowed=y
- Yeltepe, H., & İkizler, H. (2007). Egzersiz Bağımlılığı Ölçeği-21’in Türkçe geçerlilik ve güvenilirlik çalışması. Bağımlılık Dergisi, 8(1), 29-35.
- Yorulmaz, O., Inozu, M., Clark, D. A., & Radomsky, A. S. (2015). Psychometric properties of the obsessive-compulsive Inventory-Revised in a Turkish analogue sample. Psychological Reports, 117(3), 781-793. https://doi.org/10.2466/08.PR0.117c25z4
- Zeulner, B., Ziemainz, H., Beyer, C., Hammon, M., & Janka, R. (2016). Disordered eating and exercise dependence in endurance athletes. Advances in Physical Education, 6(2), 76-87. https://doi.org/10.4236/ape.2016.62009
License
Copyright (c) 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.